Do you manage the renal impact of #covid19 on general wards?
My summarised recommendations on;
✅ AKI
✅ Volume status
✅ ACEi
✅ Transplant & dialysis patients
taken from @RenalAssoc, #eraedta, #nephjc & @UpToDate
= lots of relevant info in 8 tweets👇
#medtwitter #covid4mds
My summarised recommendations on;
✅ AKI
✅ Volume status
✅ ACEi
✅ Transplant & dialysis patients
taken from @RenalAssoc, #eraedta, #nephjc & @UpToDate
= lots of relevant info in 8 tweets👇
#medtwitter #covid4mds
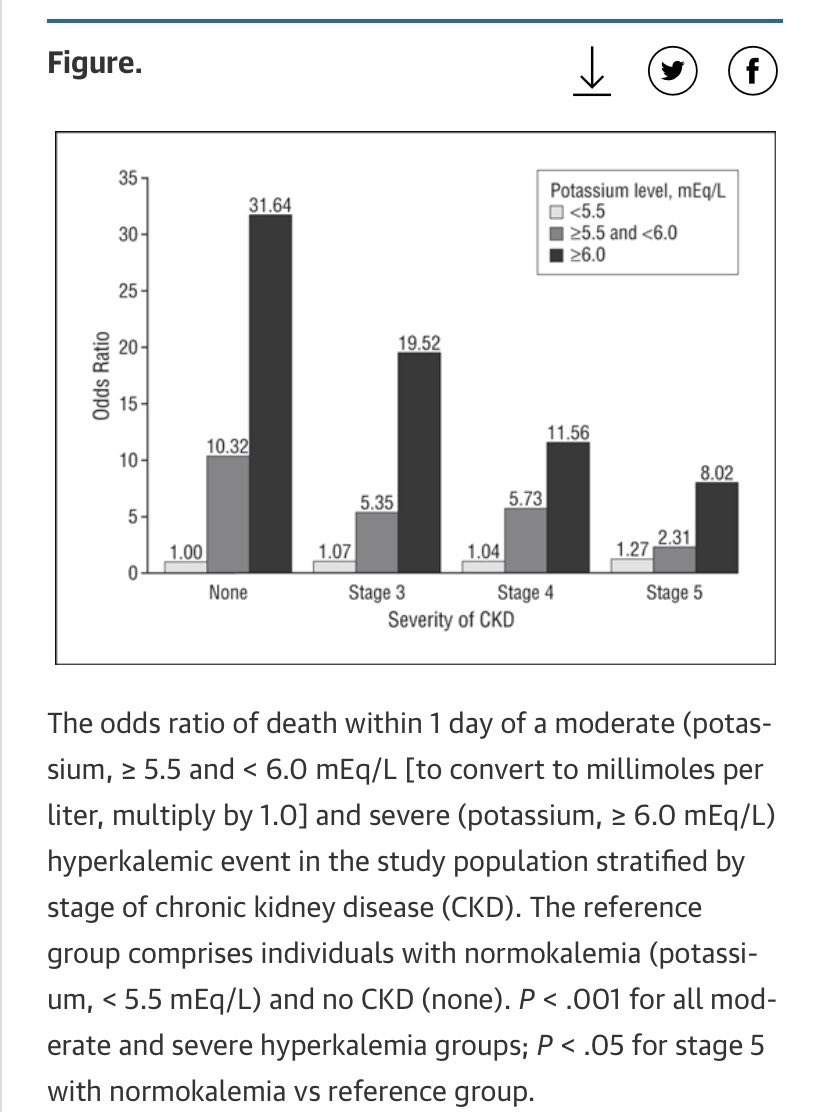
AKI 1
✅ Many potential factors;
✔️hypovolaemia due to fever / GI symptoms
✔️sepsis & cytokine release
✔️rhabdo, even without myalgia; check CK!
✔️direct viral tubule invasion?
✅ Low grade proteinuria & haematuria common
✅ Don’t miss ‘usual’ post-renal AKI; bladder scan +- US
✅ Many potential factors;
✔️hypovolaemia due to fever / GI symptoms
✔️sepsis & cytokine release
✔️rhabdo, even without myalgia; check CK!
✔️direct viral tubule invasion?
✅ Low grade proteinuria & haematuria common
✅ Don’t miss ‘usual’ post-renal AKI; bladder scan +- US
Volume status
Assessment not easy at best of times!
Balance of maintaining volume to prevent AKI & avoiding hypervolaemia which impairs oxygenation in ARDS
🟠 UK Renal Assoc - “target euvolaemia”
🟠 Uptodate - “fluid goals conservative as per ARDS criteria” but individualise
Assessment not easy at best of times!
Balance of maintaining volume to prevent AKI & avoiding hypervolaemia which impairs oxygenation in ARDS
🟠 UK Renal Assoc - “target euvolaemia”
🟠 Uptodate - “fluid goals conservative as per ARDS criteria” but individualise


AKI in #covid19 2
✅ Treat pre-renal element of AKI but be aware (as always) that thoughtless iv fluid is dangerous drug
‼️Don’t expect iv salty water to magically heal ATN - give fluid to euvolaemia then stop, even if still oligoanuric‼️
✅ Usual indications to start dialysis
✅ Treat pre-renal element of AKI but be aware (as always) that thoughtless iv fluid is dangerous drug
‼️Don’t expect iv salty water to magically heal ATN - give fluid to euvolaemia then stop, even if still oligoanuric‼️
✅ Usual indications to start dialysis
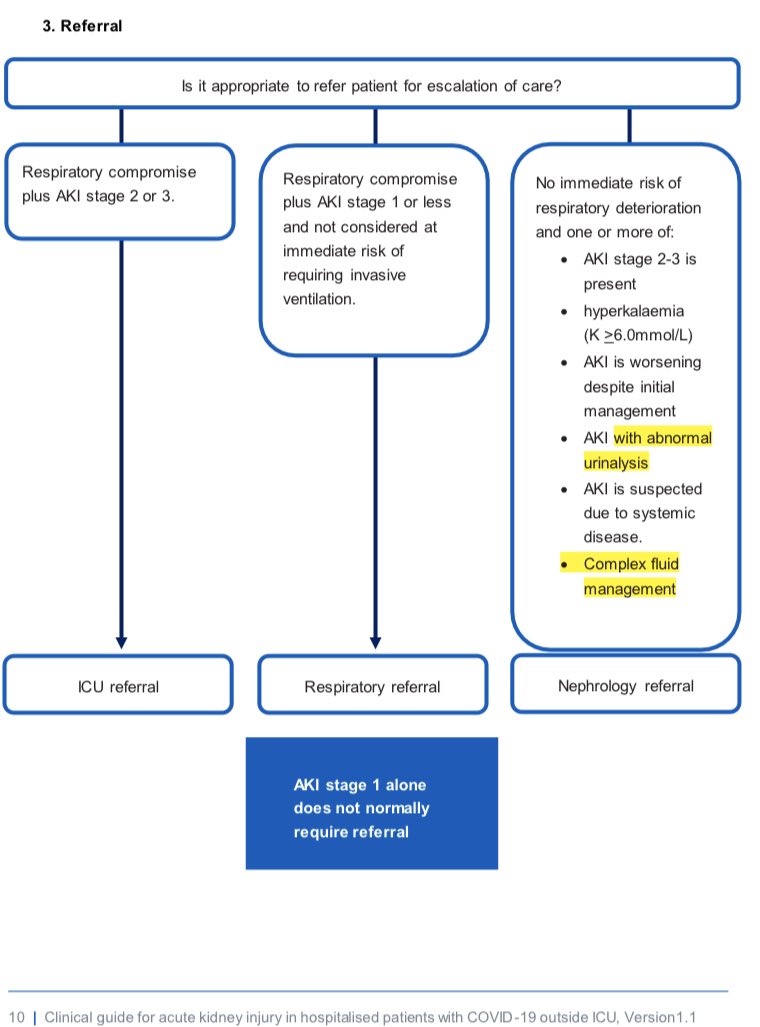
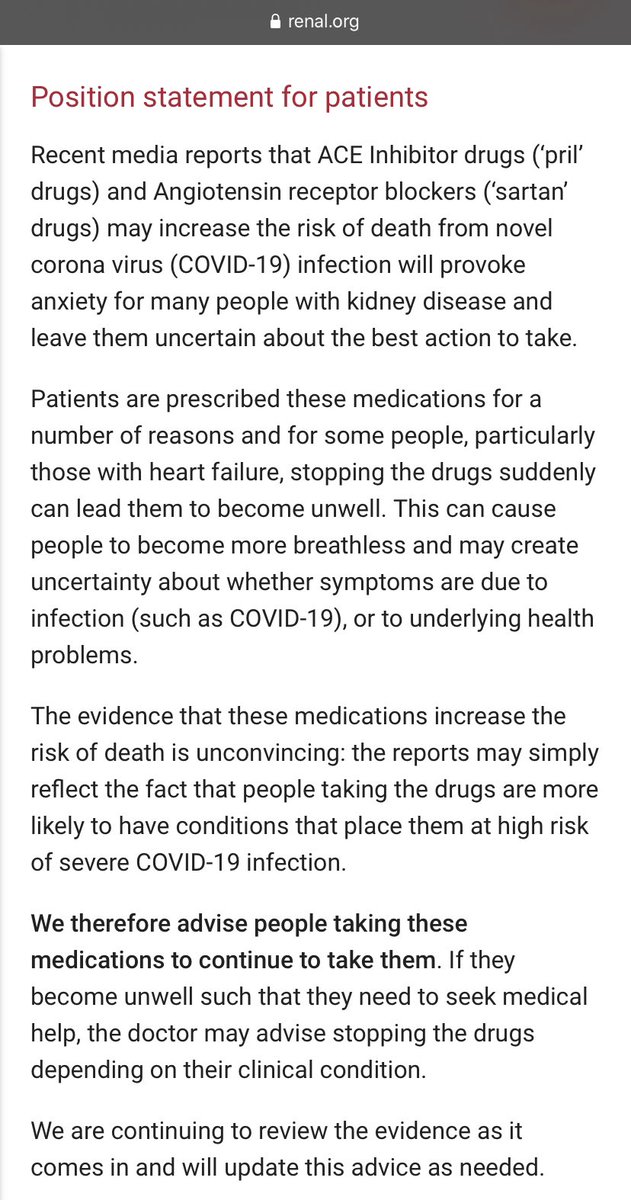
ACEi in #COVID19
☑️ All sources agree no evidence of causal harm from ACEi/ARB, so business as usual.
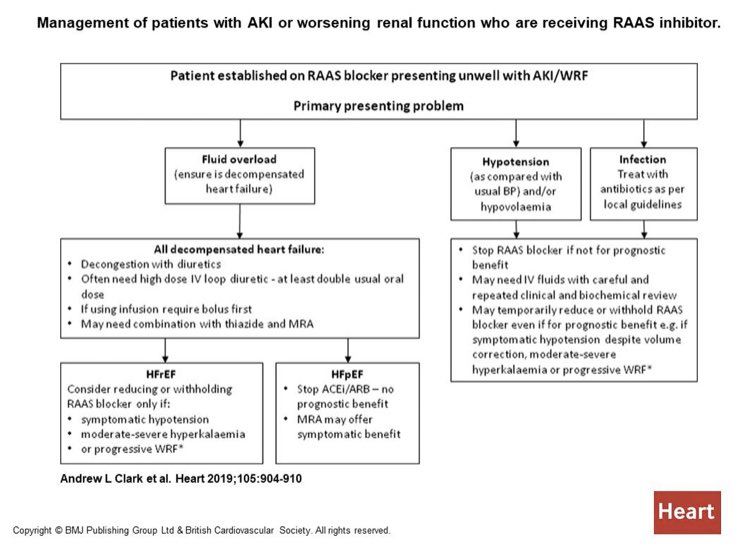
Suspend if good reason; ⬆️K, ⬇️BP, AKI (see algorithm 2nd photo)
☑️ If suspend ACEi when used for excellent indication (eg. heart failure with ⬇️EF) need a robust review plan
☑️ All sources agree no evidence of causal harm from ACEi/ARB, so business as usual.
Suspend if good reason; ⬆️K, ⬇️BP, AKI (see algorithm 2nd photo)
☑️ If suspend ACEi when used for excellent indication (eg. heart failure with ⬇️EF) need a robust review plan
Renal transplant in COVID
👉 patients seem to present typically, despite initial concern they may not
👉 consider differential diagnosis (CMV, PJP, fluid overload etc)
👉 avoid clarithromycin as CAP cover if on CNI (tacrolimus or ciclosporin) as will ⬆️⬆️levels #tipsfornewdocs
👉 patients seem to present typically, despite initial concern they may not
👉 consider differential diagnosis (CMV, PJP, fluid overload etc)
👉 avoid clarithromycin as CAP cover if on CNI (tacrolimus or ciclosporin) as will ⬆️⬆️levels #tipsfornewdocs
Transplant 2
👍 Rule of thumb - if COVID positive but disease mild;
🔴 Stop antiproliferative (MMF/AZA/mTORi)
🟠 Review CNI target levels
🟢 Continue steroid
🔴 If severe disease or particularly high risk, consider stopping CNI
🆘 As ever, involve transplant team early!
👍 Rule of thumb - if COVID positive but disease mild;
🔴 Stop antiproliferative (MMF/AZA/mTORi)
🟠 Review CNI target levels
🟢 Continue steroid
🔴 If severe disease or particularly high risk, consider stopping CNI
🆘 As ever, involve transplant team early!
Dialysis patients
⛔️ In-centre haemodialysis pts on “extremely vulnerable” list & must attend unit 3 times/week
⛔️ Higher chance atypical presentation
👉 therefore significantly lower your testing threshold
👉 if testing let HD unit know ASAP as affects cohorting, transport etc
⛔️ In-centre haemodialysis pts on “extremely vulnerable” list & must attend unit 3 times/week
⛔️ Higher chance atypical presentation
👉 therefore significantly lower your testing threshold
👉 if testing let HD unit know ASAP as affects cohorting, transport etc
NSAIDs
✅ All agree no good evidence of excess harm in COVID - but odd to mention at all as most nephrologists dislike them on a good day!
Bonus
👍 Not in recommendations but yesterday saw my new favourite algorithm for emergency CT scanning with contrast in AKI/CKD, follow it👇
✅ All agree no good evidence of excess harm in COVID - but odd to mention at all as most nephrologists dislike them on a good day!
Bonus
👍 Not in recommendations but yesterday saw my new favourite algorithm for emergency CT scanning with contrast in AKI/CKD, follow it👇
Proviso; most based on expert opinion & subject to change as facts come in!
References;
AKI
england.nhs.uk/coronavirus/pu…
ACEi
renal.org/covid-19/ra-re…
Transplant
bts.org.uk/wp-content/upl…
era-edta.org/en/wp-content/…
Nephjc (lots of great COVID kidney stuff)
nephjc.com/covid19
References;
AKI
england.nhs.uk/coronavirus/pu…
ACEi
renal.org/covid-19/ra-re…
Transplant
bts.org.uk/wp-content/upl…
era-edta.org/en/wp-content/…
Nephjc (lots of great COVID kidney stuff)
nephjc.com/covid19