1/
#medtwitter is fairly comfortable managing “normal” DKA right? But how about in the anuric dialysis patient? The cookbook protocol can be deadly.
Read this #tweetorial to learn about how their DKA pathophysiology is fascinatingly different.
#meded #nephpearls #endotwitter
#medtwitter is fairly comfortable managing “normal” DKA right? But how about in the anuric dialysis patient? The cookbook protocol can be deadly.
Read this #tweetorial to learn about how their DKA pathophysiology is fascinatingly different.
#meded #nephpearls #endotwitter
2/
Quick recap of normal DKA pathophysiology;
🔑 insulin requirement > insulin supply
✅ “stress hormones” rise
✅ blood glucose rises & because glucose is an osmotic diuretic, there is a huge, inappropriate urine output
✅ body makes ketones as alternative fuel, so pH falls
Quick recap of normal DKA pathophysiology;
🔑 insulin requirement > insulin supply
✅ “stress hormones” rise
✅ blood glucose rises & because glucose is an osmotic diuretic, there is a huge, inappropriate urine output
✅ body makes ketones as alternative fuel, so pH falls

3/
Recap of normal DKA;
✅ patient symptomatic,extracellularly dry, 6 litres down & counting
✅ whole body K low due to osmotic diuresis, but often ⬆️K at first due to hypertonicity/ low insulin/ acidosis
- serum K then rapidly falls as INsulin drives K & glucose INtracellularly
Recap of normal DKA;
✅ patient symptomatic,extracellularly dry, 6 litres down & counting
✅ whole body K low due to osmotic diuresis, but often ⬆️K at first due to hypertonicity/ low insulin/ acidosis
- serum K then rapidly falls as INsulin drives K & glucose INtracellularly
4/
Usual life-saving protocol involves treating any underlying precipitant, giving iv insulin (& usual subcut insulin) and aggressively repleting volume & electrolytes.
☠️ many protocols don’t mention that for dialysis patients this cookbook medicine can be lethal ☠️
Usual life-saving protocol involves treating any underlying precipitant, giving iv insulin (& usual subcut insulin) and aggressively repleting volume & electrolytes.
☠️ many protocols don’t mention that for dialysis patients this cookbook medicine can be lethal ☠️
5/
Patients with ⬇️GFR are actually relatively protected from DKA;
👍 decreased exogenous insulin metabolism by kidney proximal tubules = harder to be deficient
👍 in-centre haemodialysis patients seen 3 times a week = earlier illness recognition (despite being less symptomatic)
Patients with ⬇️GFR are actually relatively protected from DKA;
👍 decreased exogenous insulin metabolism by kidney proximal tubules = harder to be deficient
👍 in-centre haemodialysis patients seen 3 times a week = earlier illness recognition (despite being less symptomatic)
6/
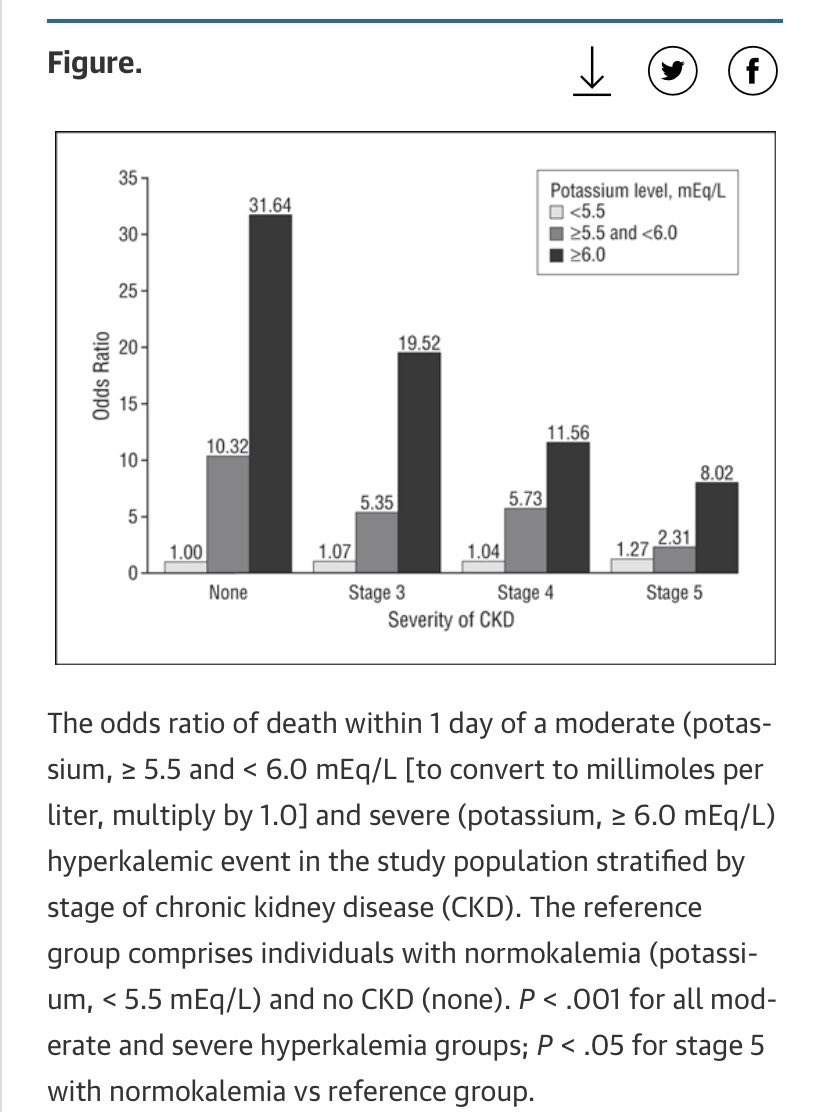
But dialysis patients do sometimes go into DKA, & are at ⬆️risk of;
❗️severe hyperkalaemia (limited K excretion)
❗️serious underlying drivers (big two here are ischaemia & infection)
❗️rapid fall in glucose with treatment = higher risk of hypoglycaemia and large tonicity swing
But dialysis patients do sometimes go into DKA, & are at ⬆️risk of;
❗️severe hyperkalaemia (limited K excretion)
❗️serious underlying drivers (big two here are ischaemia & infection)
❗️rapid fall in glucose with treatment = higher risk of hypoglycaemia and large tonicity swing
7/
However the key difference in chronically anuric dialysis patient in DKA is...
🔴 no huge osmotic diuresis 🔴
Therefore;
✅ higher initial serum glucose level (as no glycosuria)
✅ removes need for large volume & electrolyte resuscitation
⚠️ hence not for ‘the protocol’ ⚠️
However the key difference in chronically anuric dialysis patient in DKA is...
🔴 no huge osmotic diuresis 🔴
Therefore;
✅ higher initial serum glucose level (as no glycosuria)
✅ removes need for large volume & electrolyte resuscitation
⚠️ hence not for ‘the protocol’ ⚠️
8/
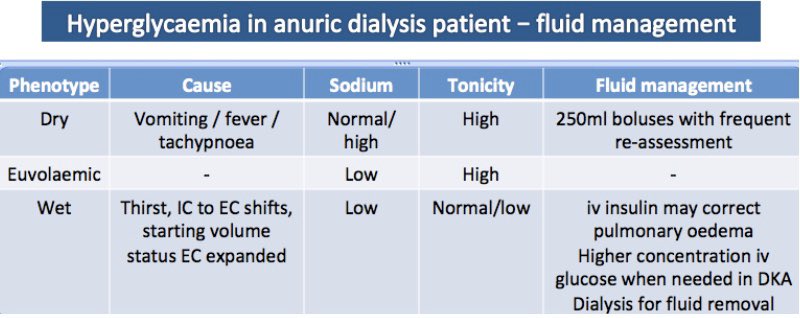
Tzamaloukas 2008 proposed 3 anuric hyperglycaemia phenotypes to help frame managing volume status
1. Dry anuric patient
- due to ⬆️RR/fever/vomiting
- high tonicity, normal/high Na
👉 Mx includes 250ml boluses
2. Euvolaemia
- high tonicity, low Na
👉 Fixes with iv insulin
Tzamaloukas 2008 proposed 3 anuric hyperglycaemia phenotypes to help frame managing volume status
1. Dry anuric patient
- due to ⬆️RR/fever/vomiting
- high tonicity, normal/high Na
👉 Mx includes 250ml boluses
2. Euvolaemia
- high tonicity, low Na
👉 Fixes with iv insulin
9/
Phenotype 3 (most interesting)
intracellular to extracellular water movement (>2L) due to ⬆️⬆️extracellular glucose & tonicity
+
huge THIRST due to same
+
zero osmotic diuresis
=
extracellularly HYPERvolaemic DKA
(with associated hypertension++ and pulmonary oedema)
Phenotype 3 (most interesting)
intracellular to extracellular water movement (>2L) due to ⬆️⬆️extracellular glucose & tonicity
+
huge THIRST due to same
+
zero osmotic diuresis
=
extracellularly HYPERvolaemic DKA
(with associated hypertension++ and pulmonary oedema)
10/
❗️This is a rather unusual type of pulmonary oedema - it is reversible with iv insulin alone ❗️
(when insulin drives glucose into cells water follows from interstitium = less extracellular water = resolution of pulmonary oedema)
❗️This is a rather unusual type of pulmonary oedema - it is reversible with iv insulin alone ❗️
(when insulin drives glucose into cells water follows from interstitium = less extracellular water = resolution of pulmonary oedema)
11/
Its well reported that hyperglycaemia causes pulmonary oedema in dialysis patients via these mechanisms even in absence of pre-existing heart disease
This may be even more likely in DKA state due to;
☑️ altered pulmonary capillary permeability
☑️ acute myocardial dysfunction
Its well reported that hyperglycaemia causes pulmonary oedema in dialysis patients via these mechanisms even in absence of pre-existing heart disease
This may be even more likely in DKA state due to;
☑️ altered pulmonary capillary permeability
☑️ acute myocardial dysfunction
12/
Other facts about the wet patient in phenotype 3;
👉 Normal initial tonicity provides (insensitive) indirect indication of high fluid consumption in anuric hyperglycaemia.
👉 severity increases with higher initial glucose levels & if volume state uncontrolled to begin with.
Other facts about the wet patient in phenotype 3;
👉 Normal initial tonicity provides (insensitive) indirect indication of high fluid consumption in anuric hyperglycaemia.
👉 severity increases with higher initial glucose levels & if volume state uncontrolled to begin with.
13/
Treatment recommendations for DKA in dialysis cohort are based on case reports;
✅ iv insulin
✅ critical care level monitoring of electrolytes, glucose & volume state
✅ be aware of ⬆️hypo risk (especially associated with insulin bolus in case series)
✅ say no to iv bicarb
Treatment recommendations for DKA in dialysis cohort are based on case reports;
✅ iv insulin
✅ critical care level monitoring of electrolytes, glucose & volume state
✅ be aware of ⬆️hypo risk (especially associated with insulin bolus in case series)
✅ say no to iv bicarb
14/
Treatment (cont)
✅ small fluid boluses with re-assessment if hypovolaemic
✅ if hypervolaemic, go with higher concentrations of iv glucose when the sugars fall
✅ caution with K replacement
✅ high index suspicion for infective / ischaemic precipitants
Treatment (cont)
✅ small fluid boluses with re-assessment if hypovolaemic
✅ if hypervolaemic, go with higher concentrations of iv glucose when the sugars fall
✅ caution with K replacement
✅ high index suspicion for infective / ischaemic precipitants
15/
Big obvious question is; given the anuric patient in DKA is often hyperkalaemic, volume overloaded & acidotic - doesn’t dialysis just fix all those things?
As you’d expect there’s no good evidence on potential harms, or whether early or late dialysis strategy best.
Big obvious question is; given the anuric patient in DKA is often hyperkalaemic, volume overloaded & acidotic - doesn’t dialysis just fix all those things?
As you’d expect there’s no good evidence on potential harms, or whether early or late dialysis strategy best.
16/
Clearly if hyperK or volume overload is life-threatening then easier decision.
Potential downsides to early HD;
❌ doesn’t fix underlying pathophysiology of insulin deficiency (if anything dialyse out insulin)
❌ masks severity
❌ cerebral oedema risk from tonicity swing
Clearly if hyperK or volume overload is life-threatening then easier decision.
Potential downsides to early HD;
❌ doesn’t fix underlying pathophysiology of insulin deficiency (if anything dialyse out insulin)
❌ masks severity
❌ cerebral oedema risk from tonicity swing
17/
Key learning points aren’t anything about anuric DKA - you may never see this.
It’s that the rules are always different in dialysis patients. Treatments are less tried and tested. Evidence base = case reports. Familiar protocols can become dangerous. Call for help early.
Key learning points aren’t anything about anuric DKA - you may never see this.
It’s that the rules are always different in dialysis patients. Treatments are less tried and tested. Evidence base = case reports. Familiar protocols can become dangerous. Call for help early.
Fin/
As ever, I’m a trainee so any disagreements / criticism / sharing experience much appreciated.
References;
sciencedirect.com/science/articl…
ncbi.nlm.nih.gov/m/pubmed/67652…
cambridge.org/core/services/…
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
As ever, I’m a trainee so any disagreements / criticism / sharing experience much appreciated.
References;
sciencedirect.com/science/articl…
ncbi.nlm.nih.gov/m/pubmed/67652…
cambridge.org/core/services/…
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…