1/ Happy July 1st! I remember my intern year getting a lot of pages & struggling to work through them. Overtime, I saw the patterns & took notes... so I present to you: Common Intern Calls
(Yes - as an intern I didn't know how to forward the pagers)
#FOAMed #MedTwitter #July1st
(Yes - as an intern I didn't know how to forward the pagers)
#FOAMed #MedTwitter #July1st
2/ This isn't an exhaustive list-but illustrative examples of common surgery intern calls. An upfront take home message, you'll rarely go wrong if you:
1. Get more Data - repeat vitals, labs
2. See the patient - sick? not sick?
3. Pass it up - get a senior involved when unsure
1. Get more Data - repeat vitals, labs
2. See the patient - sick? not sick?
3. Pass it up - get a senior involved when unsure

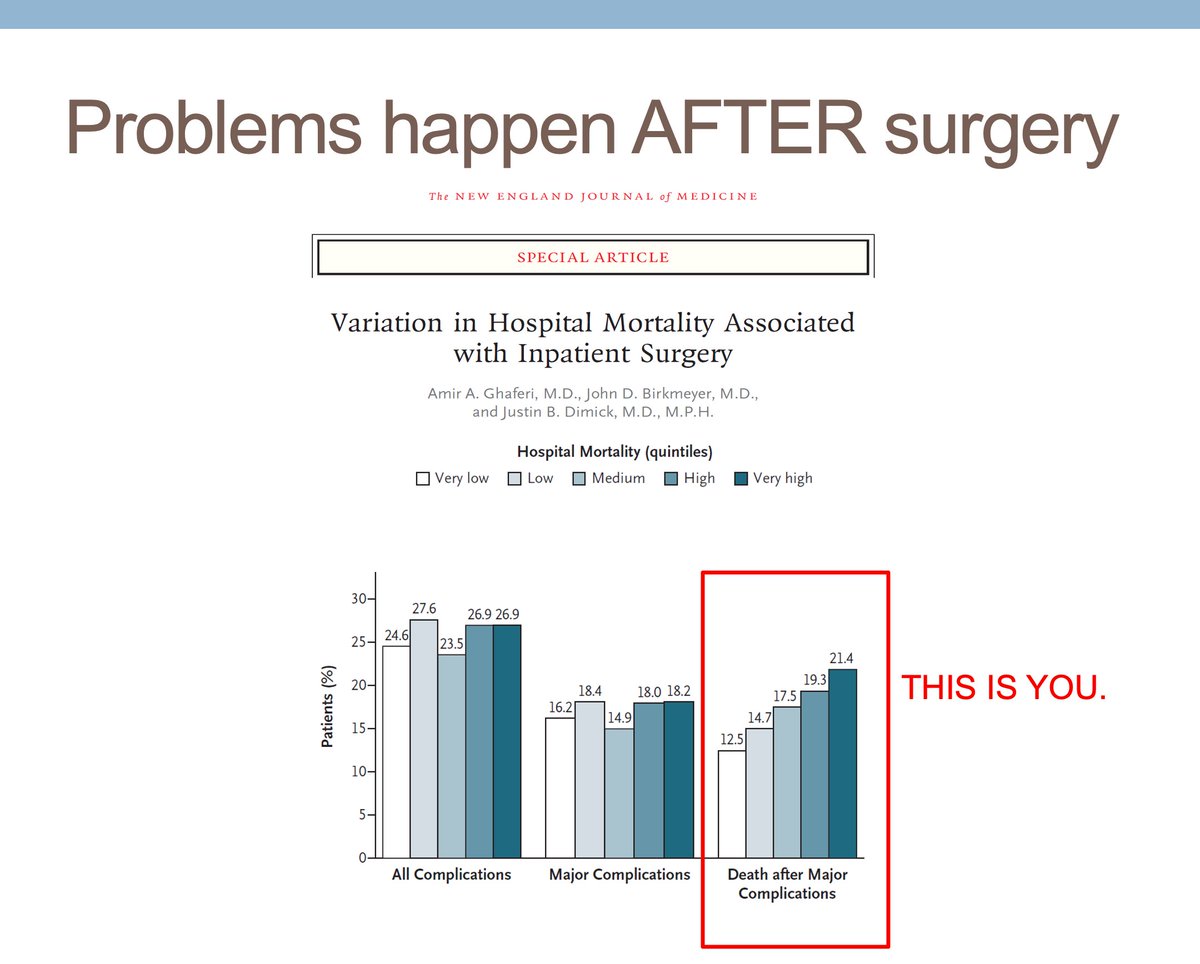
3 / Some context: As the landmark work led by @AmirGhaferi demonstrated, variation in surgical mortality is influenced by our ability to recognize problems early & address them before they domino. Intern call = find the first domino & address early!
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
4/ This one is classic: "Your patient is here." Perhaps a patient not signed out to you, a transfer from OSH that came a day late once a bed was available. This will happen. Never assume it's someone else's patient because you weren't expecting it.

5/ So what to do? Perfect time to try out our take home message:
1. Get more data
2. See the patient
3. Pass it up
Will only take a minutes. If not your patient, take some time to help make sure right team is contacted.
1. Get more data
2. See the patient
3. Pass it up
Will only take a minutes. If not your patient, take some time to help make sure right team is contacted.
6/ Chest pain. Will be common and the differential is broad. At many institution, chest pain will prompt a "Rapid Response" or "Code White" (something one level less an attend than a full code.) Embrace it, its more hands on deck to help you.
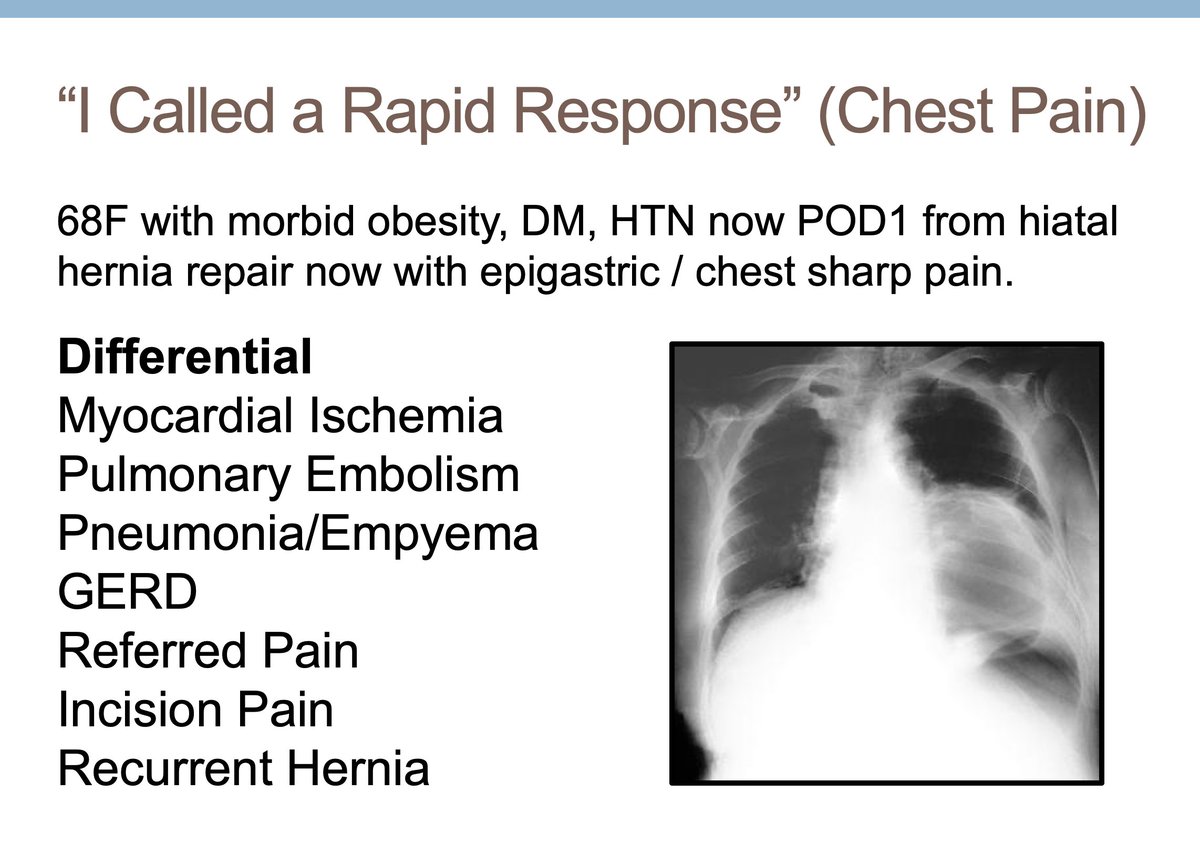
7/ Working up chest pain can be intimidating. You don't need to be a cardiologist, but you should be able to recognize if the EKG is sinus, if ST changes / T wave inversions are present.
Pro Tip: Find an old EKG and compare. Anything new / different? Probably needs more work-up.
Pro Tip: Find an old EKG and compare. Anything new / different? Probably needs more work-up.

8/ Now my favorite skill of Intern Year - efficiently updating a senior. Depending your institution / service / rotation, the person you're calling may be hearing about this patient for the first time. Here's a template to follow:

9/ Here's the chest pain example filled out. Remember, the person you're calling may not know this patient yet.
Pro Tip: Sit at a computer - they will have more questions and you can start ordering the next set of instructions.
Pro Tip: Sit at a computer - they will have more questions and you can start ordering the next set of instructions.

10/ Alright, let's keeping going. Post-operative hypoxia is very common. Didn't make the slide, but suppose current events would also put #COVID on the differential now, too.
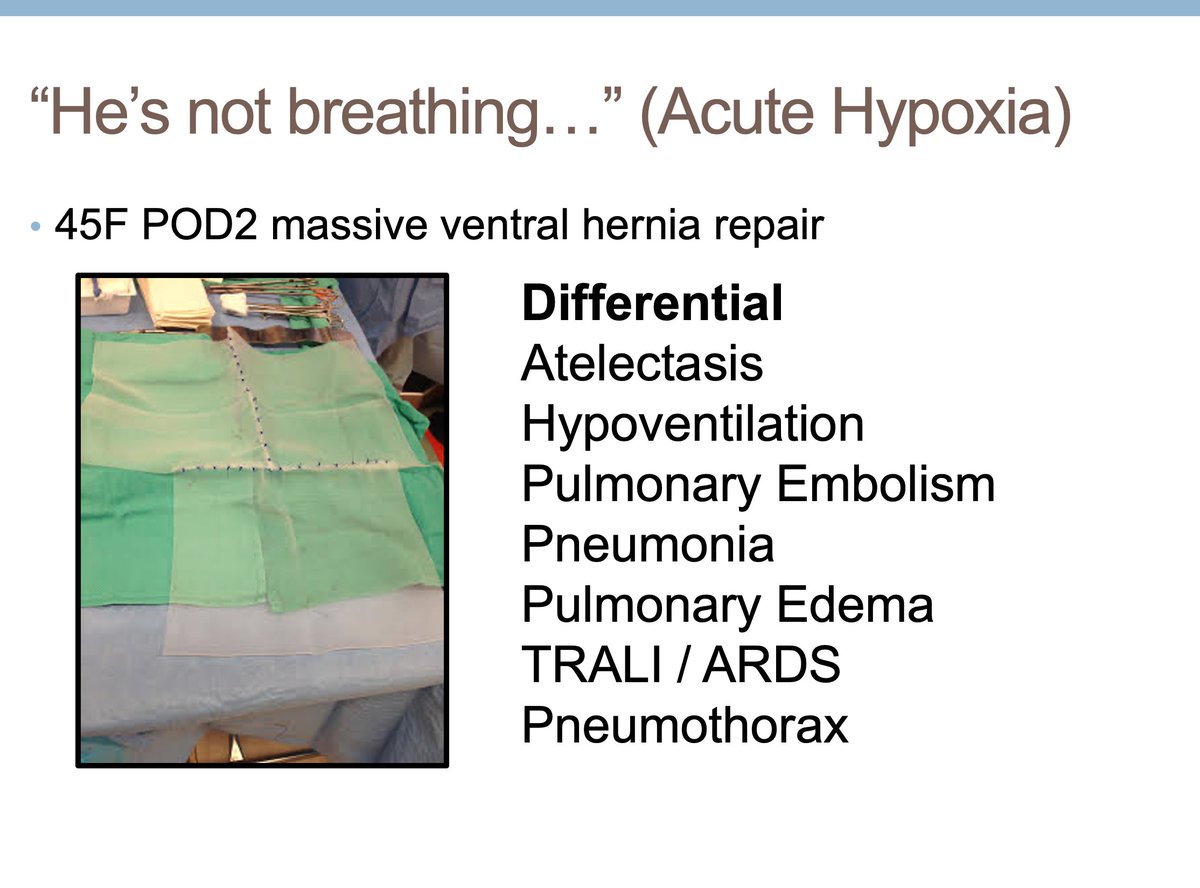
11/ Can't overstate how important it is to see the patient and do a physical exam. Won't always give you the diagnosis, but you don't want to miss something obvious (e.g. unilateral leg swelling). And yup, find that stethoscope.

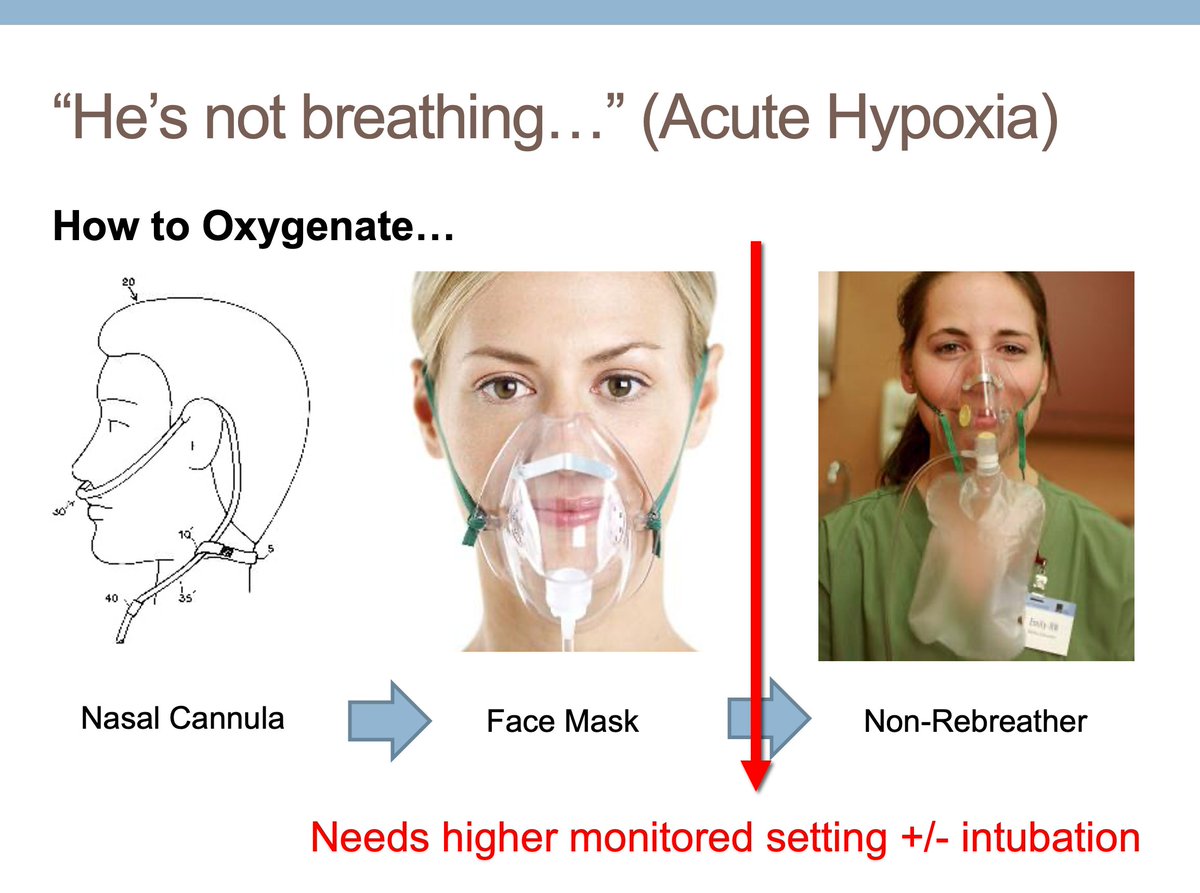
12/ Good time to learn different methods to delivery oxygen & to understand once you cross into non-rebreather, you're not far away from possibly needing intubation.
(My first call to a chief...I confused face mask & Non-rebreather...understood later why she ran to bedside...)
(My first call to a chief...I confused face mask & Non-rebreather...understood later why she ran to bedside...)
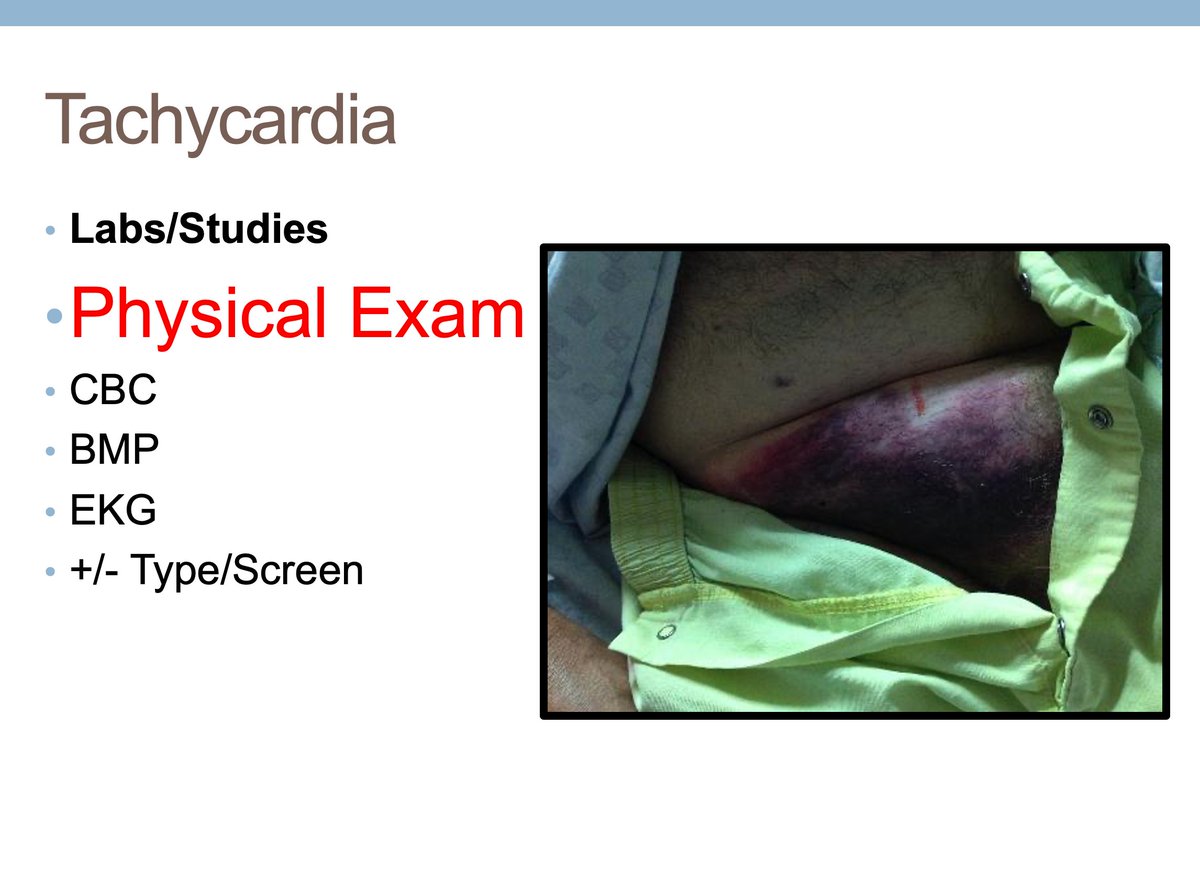
13/ Another common one - tachycardia.
Most common mistake? Hanging up after hearing the HR without getting the rest of the vitals. It's okay, you're a little nervous, we get it. But get in the habit of getting all the vitals to put the abnormal one in context.
Most common mistake? Hanging up after hearing the HR without getting the rest of the vitals. It's okay, you're a little nervous, we get it. But get in the habit of getting all the vitals to put the abnormal one in context.

14/ Sinus tachycardia differential is broad. Bleeding will always be toward the top. Resist the urge to attribute elevated heart rates to pain or anxiety. It might be, but convince yourself it not something else first.

15/ If there is any recurrent theme about common intern calls -- GO SEE THE PATIENT. Even in our tech-savy era, doing a physical exam and laying eyes on a patient will always help you.
Yup--full out groin hematoma at puncture site. Didn't have to hunt much longer for HR source.
Yup--full out groin hematoma at puncture site. Didn't have to hunt much longer for HR source.
16/ Ah yes, AFib with RVR. Every surgery intern will see this at some point. It is worth taking some time to read about it and understand it.

17/ Your response to AFib will first rely on Stable vs Unstable. General guidelines below.
Relax, as an intern you shouldn't be cardioverting alone. If needed, you should be in a more monitored setting with help!
Relax, as an intern you shouldn't be cardioverting alone. If needed, you should be in a more monitored setting with help!


18/ Home stretch of common calls... Low urine output. "Strict Ins and Outs" will be your new favorite request. Low urine output (<0.5cc/kg/hr) can be an early sign a problem in any post-op patient. In a kidney transplant? Stakes even higher!

19/ Sometimes urine output in chart isn't accurate -- patient doesn't save in urinal hat, doesn't get recorded, etc. Labs, Urinalysis can help you figure out volume status and reason for low urine output.

20/ Ok, not meant to be an exhaustive list, but hopefully going through these examples with your team will help generate good discussion and work out common scenarios. Reminder on the take home:
1. Get more Data
2. See the Patient
3. Pass it up
#FOAMED #MedTwitter
1. Get more Data
2. See the Patient
3. Pass it up
#FOAMED #MedTwitter
@threadreaderapp unroll