
Neuroanatomy TOTD #4
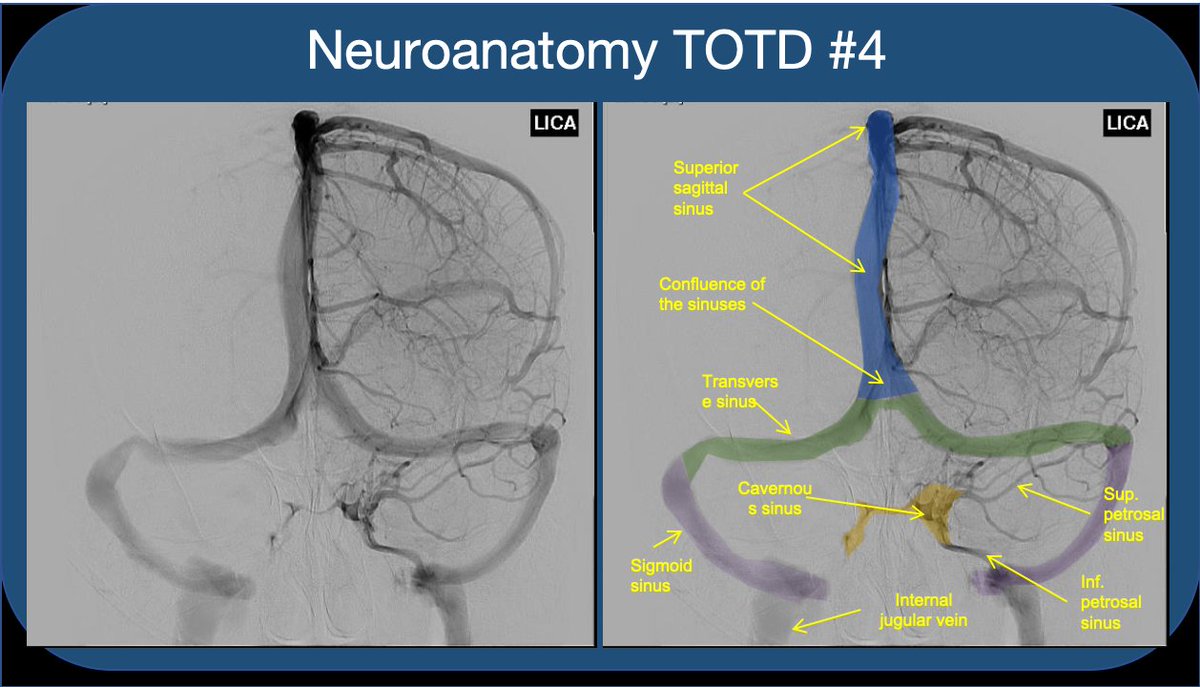
1/5 Answer: The orange structure is the cavernous sinus (CS), a paired dura-lined venous cavity on either side of the sella. The sinuses are split into numerous “caves” by fibrous septae (hence the name). #neuroanatomy #neurorad #medtwitter #neuroanatomyTOTD
1/5 Answer: The orange structure is the cavernous sinus (CS), a paired dura-lined venous cavity on either side of the sella. The sinuses are split into numerous “caves” by fibrous septae (hence the name). #neuroanatomy #neurorad #medtwitter #neuroanatomyTOTD
2/5 Note that the paired sinuses are often variably connected by “intercavernous sinuses”. While the CS is often taught for its relationship to the ICA and cranial nerves, I find that medical students and residents rarely understand the flow of blood through the sinus.
3/5 The CS receives blood from sup. and inf. ophthalmic veins draining the orbit--This is how a facial/orbital infection spreads intracranially to CS (classic #usmle ?). The sphenoparietal sinus as well as the superficial middle and inferieor cerebral veins also feed into the CS.

4/5 The CS drains via the sup & inf petrosal sinuses (to the transverse/sigmoid sinus & sigmoid/int jug), as well as variable drainage through emissary veins which course through skull foramina (like the foramen ovale). This includes variable connections to the pterygoid plexus.

5/5 Understanding crucial for interventional closure of carotid-cavernous AV fistula. Can be approached: retrograde via IJV/inf petrosal sinus, anterograde/transorbital through sup ophth vein, +/- arterial approach via ICA. #meded #FOAMed #FOAMrad #radres #radiology #neurosurgery

• • •
Missing some Tweet in this thread? You can try to
force a refresh
















