@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty 1/29 yo M, smoker, presents with RLQ abscess w fistula to the TI; he undergoes abscess drainage & then ileocecal✂️w primary ileocolonic anastomosis. Path c/w #Crohns, margins free of disease. You see him for f/up 2 weeks post-op, What's the next ? #MondayNightIBD #Back2Basics
@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty 2/ Let’s talk #Crohn’s intestinal complications
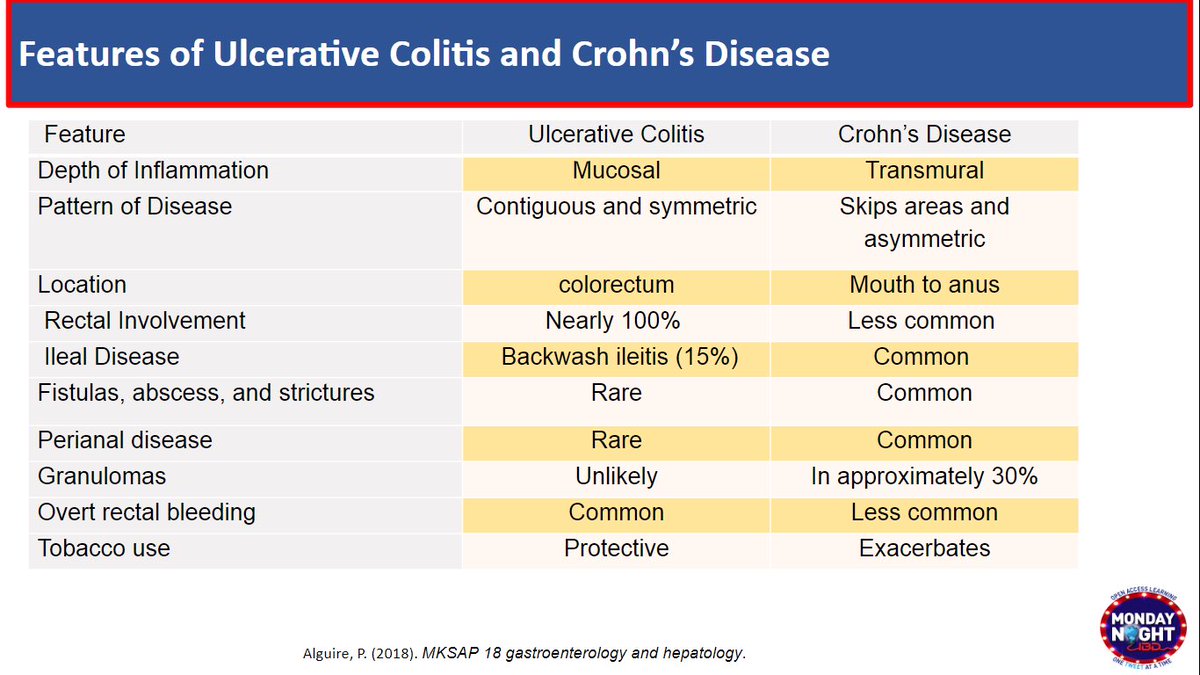
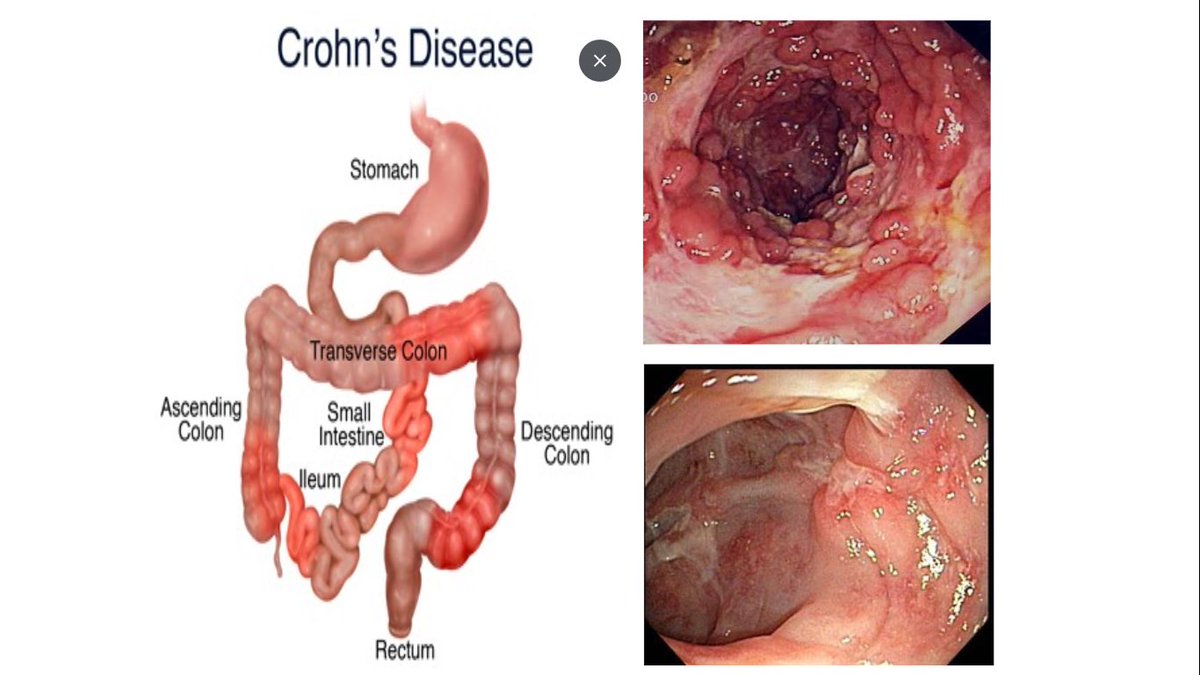
CD can present w stricturing/perforating complications
50-60% CD will develop strictures, fistulas or abscesses over time
70% require surgical✂️by 15yrs of dx
Surgery not curative, most pts will have endo recurrence 1 yr post-IC✂️
CD can present w stricturing/perforating complications
50-60% CD will develop strictures, fistulas or abscesses over time
70% require surgical✂️by 15yrs of dx
Surgery not curative, most pts will have endo recurrence 1 yr post-IC✂️

@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty 3/ Natural course of CD recurrence post- IC ✂️
📌Histologic e/o CD within 3 wks post-op !!
📌70-90% pts w endo recurrence at 1 year
📌30-60% pts w clinical recurrence by 3 & 5 yrs
📌50% will need ✂️by 5 yrs
@MRegueiroMD
📌Histologic e/o CD within 3 wks post-op !!
📌70-90% pts w endo recurrence at 1 year
📌30-60% pts w clinical recurrence by 3 & 5 yrs
📌50% will need ✂️by 5 yrs
@MRegueiroMD

@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD 4/ Post-op recurrence (POR) assessed by Endoscopy:
🚫 Rely on symptoms to define recurrence !!
🚩Endo dis often precede clinical symptoms
🚩Endo dis can be clinically silent
🚩GI symptoms post-op can be due to non-CD: bile salt diarrhea, altered motility, malabsorption, SIBO
🚫 Rely on symptoms to define recurrence !!
🚩Endo dis often precede clinical symptoms
🚩Endo dis can be clinically silent
🚩GI symptoms post-op can be due to non-CD: bile salt diarrhea, altered motility, malabsorption, SIBO
@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD 5/ Rutgeerts Score @ibdleuven :Endo recur. at ileum post- IC✂️
🚩Predictor of clinical recur.
🔺i0-i1 =Endo remission, <10% risk of clinical rec., low risk of 2nd✂️@ 5yrs
=No RX/No change in RX needed
🔺i2-i3-i4 =Endo recur.up to 90% risk for 2nd CD✂️@ 5yrs
=Need Rx/adjust Rx
🚩Predictor of clinical recur.
🔺i0-i1 =Endo remission, <10% risk of clinical rec., low risk of 2nd✂️@ 5yrs
=No RX/No change in RX needed
🔺i2-i3-i4 =Endo recur.up to 90% risk for 2nd CD✂️@ 5yrs
=Need Rx/adjust Rx

@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD 6/ Other non-invasive modalities to detect POR
(under study) →
🔺FCP→ > 150 μg/g would be those to target for an ileocolonoscopy to assess recurrence.
🔺SBUS→ >6mm bowel thickness having a 40% risk of surgical recurrence
🔺CTE/MRE→ variable correlation, need further study
(under study) →
🔺FCP→ > 150 μg/g would be those to target for an ileocolonoscopy to assess recurrence.
🔺SBUS→ >6mm bowel thickness having a 40% risk of surgical recurrence
🔺CTE/MRE→ variable correlation, need further study
@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD 7/ Who is at ⬆️ Risk for POR?
🚩Pt factors
Smoking, >15 cigs/d
Young age at time of Sx (<30yo)
🚩Disease/Sx factors:
Short dis. duration before Sx
>2 prior✂️
Penetrating dis
SB✂️>50cm
➕Disease at resection margins
🚫Effect EEA vs SSA anastomosis
ncbi.nlm.nih.gov/pmc/articles/P…
🚩Pt factors
Smoking, >15 cigs/d
Young age at time of Sx (<30yo)
🚩Disease/Sx factors:
Short dis. duration before Sx
>2 prior✂️
Penetrating dis
SB✂️>50cm
➕Disease at resection margins
🚫Effect EEA vs SSA anastomosis
ncbi.nlm.nih.gov/pmc/articles/P…

@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD @JeanDonet 8/ ⬇️Risk of POR of CD:
🔹Older patient (>50 y)
🔹Nonsmoker
🔹1st Sx for a short segment of fibrostenotic disease (<10 to 20 cm)
🔹Disease duration >10 y
🔹Older patient (>50 y)
🔹Nonsmoker
🔹1st Sx for a short segment of fibrostenotic disease (<10 to 20 cm)
🔹Disease duration >10 y
@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD @JeanDonet 9/ What therapies are proven to ⬇️ risk of POR of CD ?
🚫 5ASA or budesonide
✅AZA
✅Nitroimidazole x 3 months (consider for low risk pts)
✅✅✅ Anti-TNF
Slides👇🏼
@MRegueiroMD @AGA_Gastro doi.org/10.1053/j.gast…
@IBDJournals
doi.org/10.1002/ibd.20…
🚫 5ASA or budesonide
✅AZA
✅Nitroimidazole x 3 months (consider for low risk pts)
✅✅✅ Anti-TNF
Slides👇🏼
@MRegueiroMD @AGA_Gastro doi.org/10.1053/j.gast…
@IBDJournals
doi.org/10.1002/ibd.20…


@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD @JeanDonet @AGA_Gastro @IBDJournals 10/ When to start prophylactic Rx post-IC ✂️
🔺High risk pts
✅Start TNFi within 4 wks post-op, as long as no infection/wound complications
✅C-scope at 6-12mos to assess ileum above IC anastomosis
🔺Low risk pts
✅No Rx or Nitroimidazole x 3 months
✅C-scope at 6mos, reassess
🔺High risk pts
✅Start TNFi within 4 wks post-op, as long as no infection/wound complications
✅C-scope at 6-12mos to assess ileum above IC anastomosis
🔺Low risk pts
✅No Rx or Nitroimidazole x 3 months
✅C-scope at 6mos, reassess

@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD @JeanDonet @AGA_Gastro @IBDJournals 11/ Let's recap #MondayNightIBD #Back2Basics
🔺Risk of Endo POR ~90% @1yr
🔺Endo recur. often clinically silent
🚫 Rely on symptoms to start Rx
✅Risk stratify pt to decide on prophylaxis Rx vs surveillance
✅C-scope for Rutgeers score @6-12 mos & periodically
✅Adjust Rx prn
🔺Risk of Endo POR ~90% @1yr
🔺Endo recur. often clinically silent
🚫 Rely on symptoms to start Rx
✅Risk stratify pt to decide on prophylaxis Rx vs surveillance
✅C-scope for Rutgeers score @6-12 mos & periodically
✅Adjust Rx prn
@MondayNightIBD @ibdnaik @SobiaMujtabaMD @ibdleuven @DCharabaty @MRegueiroMD @JeanDonet @AGA_Gastro @IBDJournals @1yr @6 @Waseem_AhmedMD @DrMalSimons @EndoAthlete @MahamHayatMD @joshsteinbergMD @AsadurRahman87 @VivyTCmd @ptandonGI @javiervg0902 @eric_kauff @OmerShahabMD @EulaMD @VicentHernande9 @DVinsard @NabaSaeedQ @DrMohdZein @KM_Pawlak @HarisMD14 @purnie_mae
• • •
Missing some Tweet in this thread? You can try to
force a refresh