Elderly ♂️, PMH of T2DM and CKD.
Suspected COVID-19 because of shortness of breath. Sent to the COVID-19 ED service.
No fever, no cough. No chest pain. Physical exam with patient sitting up (almost 90°):
¿Is this neck pulse arterial or venous? 1/8
Suspected COVID-19 because of shortness of breath. Sent to the COVID-19 ED service.
No fever, no cough. No chest pain. Physical exam with patient sitting up (almost 90°):
¿Is this neck pulse arterial or venous? 1/8
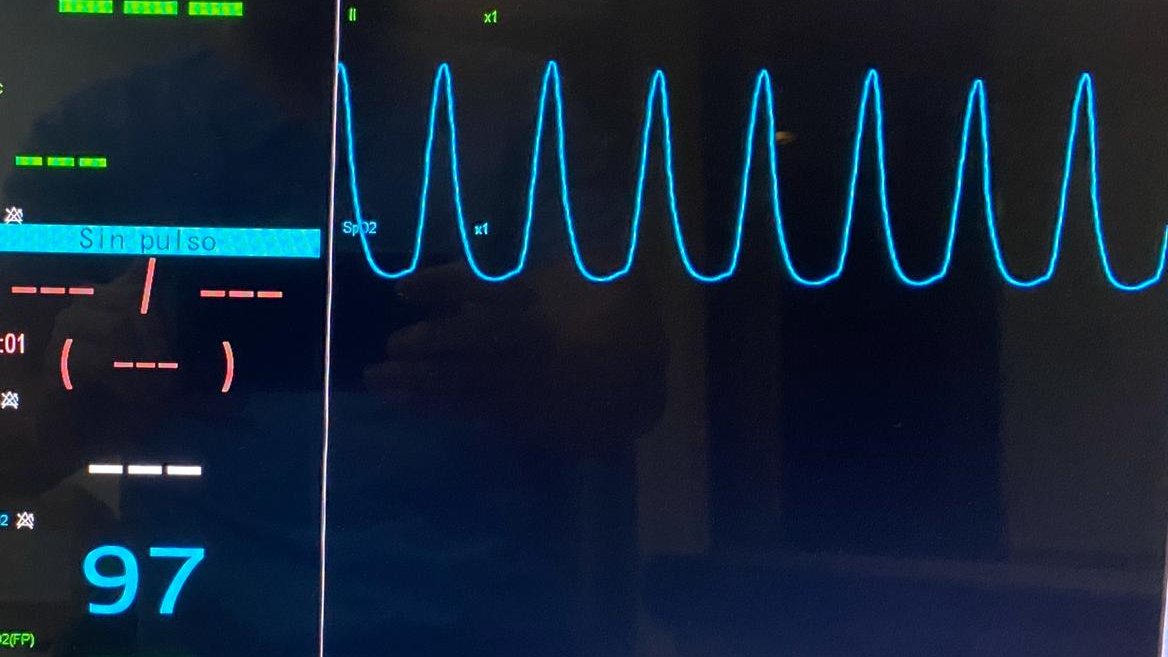
Pulse is diffuse and the most striking feature is inward movement. I borrowed this table from @AndreMansoor's must-see lecture on Jugular Venous Pulse **Curiously, notice that there is a single peak instead of the expected double peak 🤔 2/8 

I had to get my probe! #POCUS showed severely reduced EF with anterior wall motion abnormality and normal RV function.
EKG showed anterior ST segment changes. This was ACS! Cath lab was activated
3/8
EKG showed anterior ST segment changes. This was ACS! Cath lab was activated
3/8
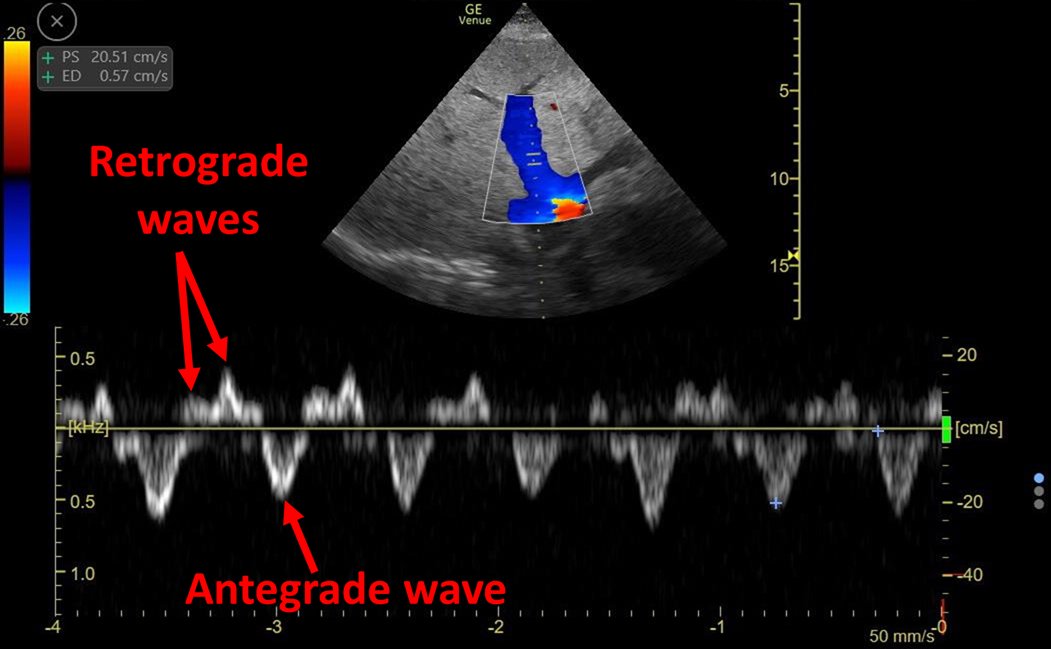
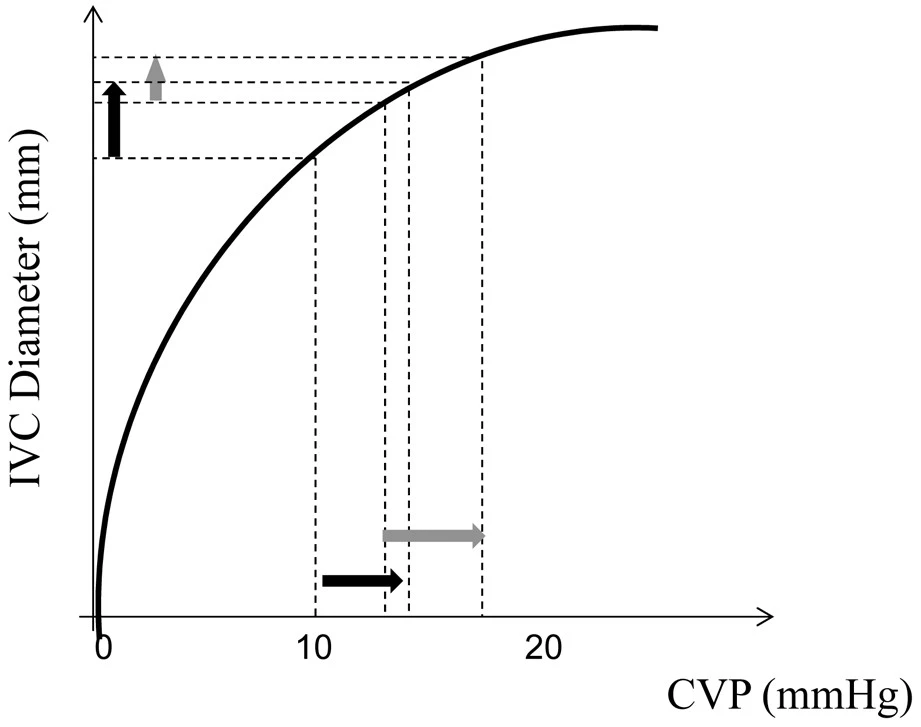
#VExUS showed plethoric IVC, reverse hepatic vein flow and portal vein with >50% pulsatility.
#VExUS = 3
Hepatic vein Doppler flow reversal explains why there was only ONE peak on JVP. There is only one antegrade wave!
4/8
#VExUS = 3
Hepatic vein Doppler flow reversal explains why there was only ONE peak on JVP. There is only one antegrade wave!
4/8
🚨Next is for Doppler nerds only:
NO ECG on #POCUS machine available to determine the origin of flow reversal on HV.
So, it could either be S wave reversal or D wave reversal. **Patient was in sinus rhythm 5/8
NO ECG on #POCUS machine available to determine the origin of flow reversal on HV.
So, it could either be S wave reversal or D wave reversal. **Patient was in sinus rhythm 5/8

S wave reversal is only observed in cases of severe RV disfunction or severe tricuspid regurgitation... None were present: 6/8
So this leads me to speculate that septal motion during LV DIASTOLE is impeding RV filling.
Given anterior wall was completely akinetic, there was septal bulging into the RV in diastole:
So I believe HV shows D wave reversal! ping @NephroP @Thind888 @msenussiMD
7/8
Given anterior wall was completely akinetic, there was septal bulging into the RV in diastole:
So I believe HV shows D wave reversal! ping @NephroP @Thind888 @msenussiMD
7/8
In conclusion:
-This was not COVID-19
-Physical exam rules!
-#POCUS definitely enhanced examination
-Single peak on JVP suggests flow reversal (either X or Y descent is missing)
-This may be an interesting cause of diastolic wave reversal on hepatic vein doppler
8/8
-This was not COVID-19
-Physical exam rules!
-#POCUS definitely enhanced examination
-Single peak on JVP suggests flow reversal (either X or Y descent is missing)
-This may be an interesting cause of diastolic wave reversal on hepatic vein doppler
8/8
• • •
Missing some Tweet in this thread? You can try to
force a refresh