Dr. Jardine on side effects of SGLT2i. Where is evidence coming from? #Kidneywk 
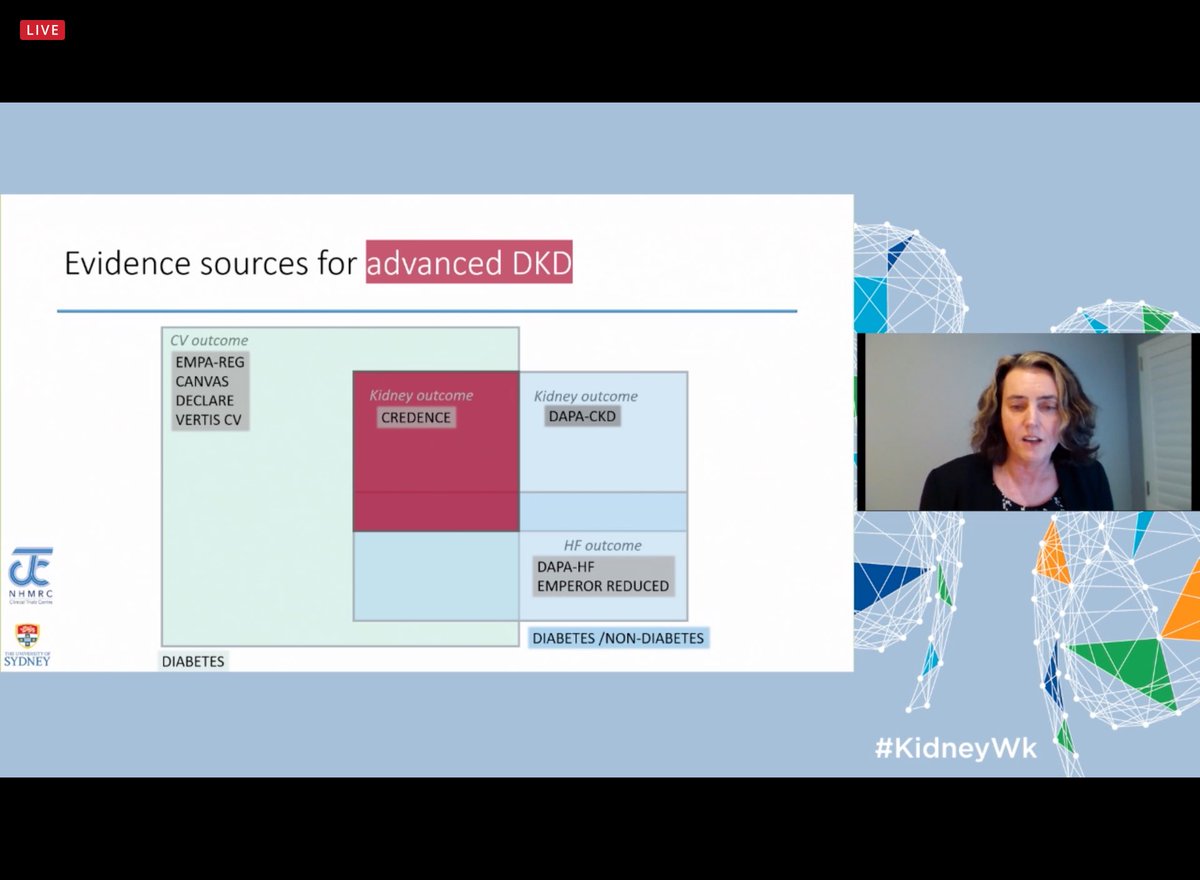
Mostly is coming from CREDECE since it has the largest population of advanced CKD. Side effects are not different across different stages of CKD #Kidneywk


Hypoglycaemia not common, about 1%. DKA is rare (1 case per 1000 users) but real mostly seen in people who require insulin. #kidneywk




Some of the characteristics of DKA associated with SGLT2i . The most striking ones are lowish glucose levels and its association with fasting. Implementation of sick day rules may prevent some of these cases #Kidneywk




Amputations were only significant in #CANVAS. The major risk factor is history of another amputation. #CREDECE modified its protocol to reduce this risk. #Kidneywk



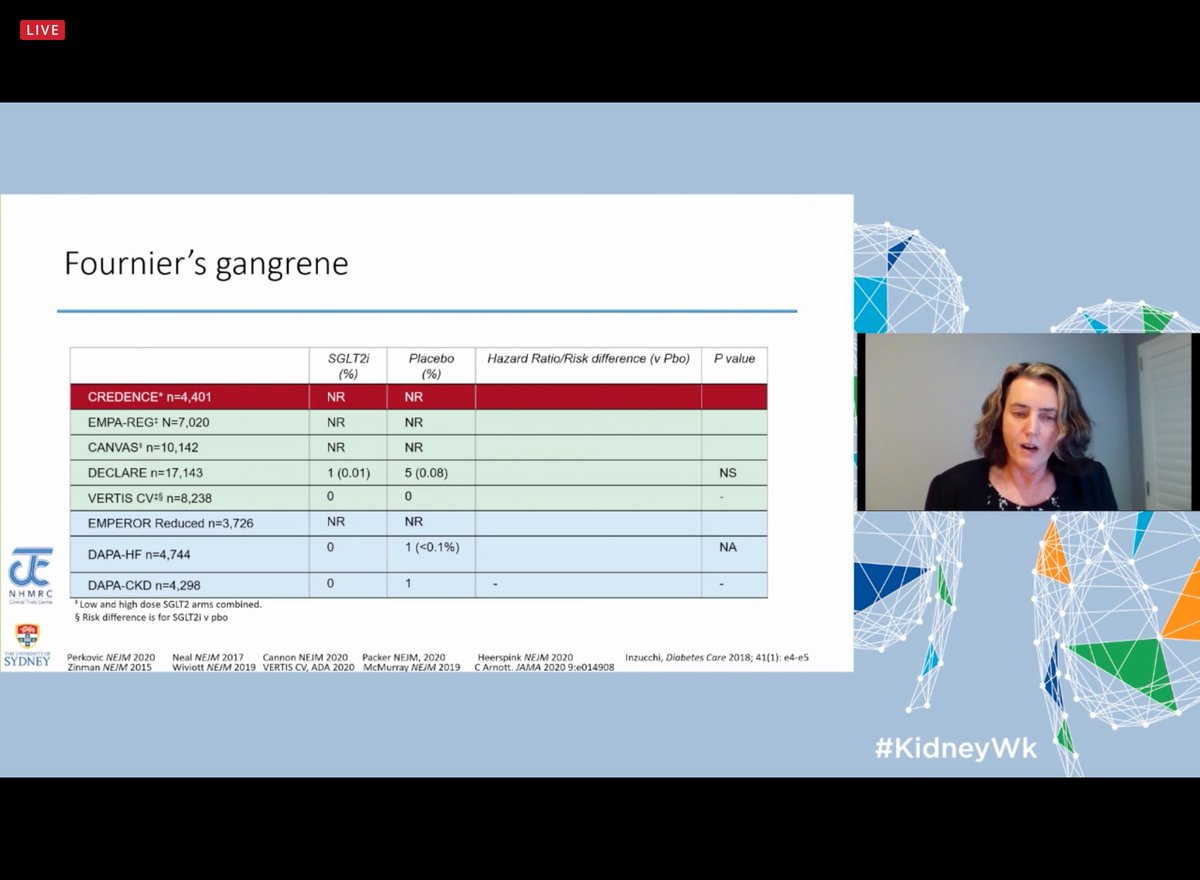
Fourniers Gangrene is very rare. Real world data was maybe driven for increased scrutiny of the new drugs. It remained a very rare event. 5.2/100000 persons years. Actually the risk may be even lower for people on #SGLT2i #kidneywk @drjjw


Volume depletion was not found int the clinical trials. No difference in UTIs . Having one is not associated with having another #Kidneywk




Mycotic infections are common in people with DM. Not a reason for stopping these drugs. #Kidneywk


The initial drop in GFR is not AKI and it is 100% reversible and has no prognostic significance. #kidneywk




Patients with GFR <30 may also have benefits from using these drugs with no increase of adverse events. #KidneyWk


What to do during first assessment after initiating #SGLT2i and more wisdom from trials + sick day rules. Continue the drug until the patient reaches RRT!!! #Kidneywk



• • •
Missing some Tweet in this thread? You can try to
force a refresh