
Comparison of SPI-M medium term projections for England hospitalisations/deaths and subsequent data has now been published (along with some model descriptions):
assets.publishing.service.gov.uk/government/upl… 1/
assets.publishing.service.gov.uk/government/upl… 1/


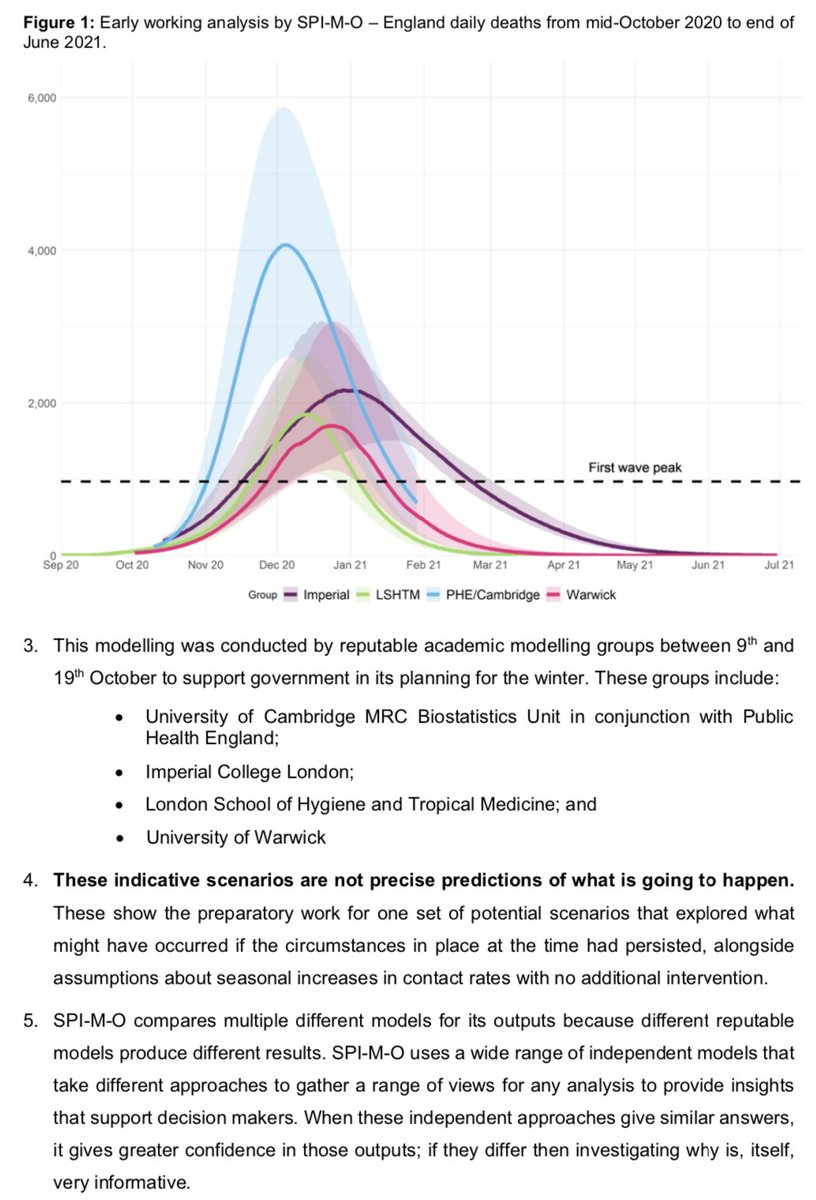
Additional context on that early working analysis also now available (noting that unlike above, these were *scenarios* to illustrate a reasonable worst case without further interventions, not forecasts): assets.publishing.service.gov.uk/government/upl… 2/

More on how to evaluate forecasts:
https://twitter.com/AdamJKucharski/status/1319955668812599296?s=20
Finally, credit to my colleagues around the UK who have been working flat out on this sort of analysis for months (often around other full-time commitments) and who are still working as hard as they can to get more of their analysis/code out there.
• • •
Missing some Tweet in this thread? You can try to
force a refresh




