My discussion on the role schools play in transmission, and what needs to be done with @bbcworldservice - speaking with Paul Henley and panelists, @georginagodwin and @DomJermey. Please listen from 30:00 onwards.
A thread on the evidence discussed👇
bbc.co.uk/sounds/play/w1…
A thread on the evidence discussed👇
bbc.co.uk/sounds/play/w1…
Are children susceptible to transmission?
Yes - overwhelming evidence that children get infected.
Are they as susceptible as adults?
Difficult to say, as getting infection is a composite of exposure- no. of contacts, as well as susceptibility to infection.
Yes - overwhelming evidence that children get infected.
Are they as susceptible as adults?
Difficult to say, as getting infection is a composite of exposure- no. of contacts, as well as susceptibility to infection.
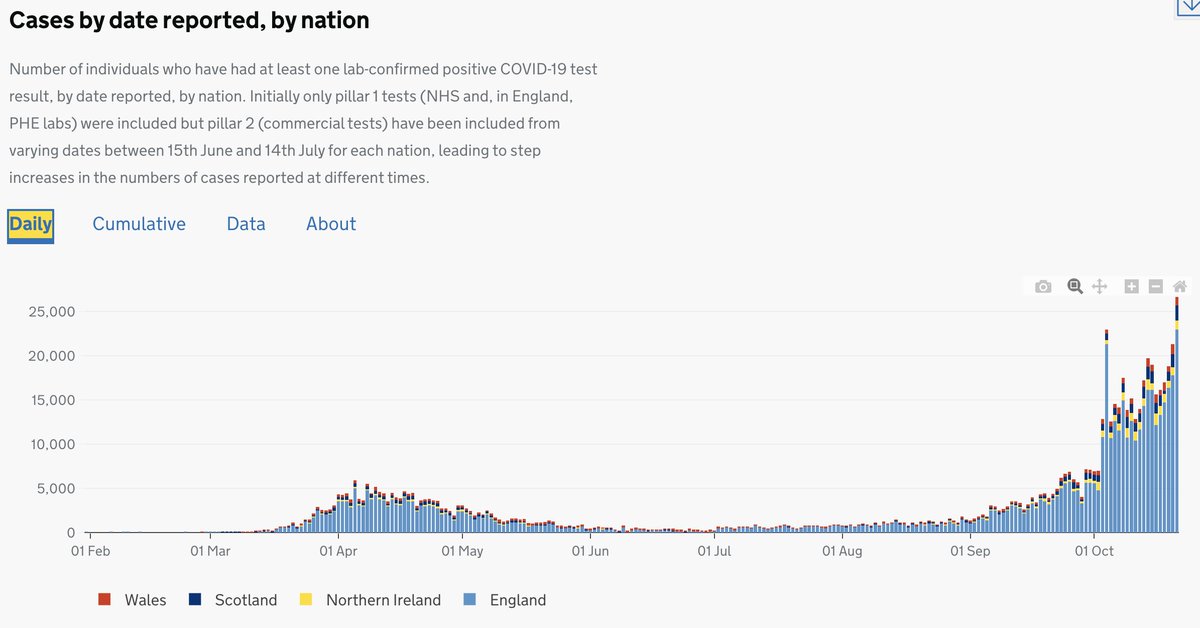
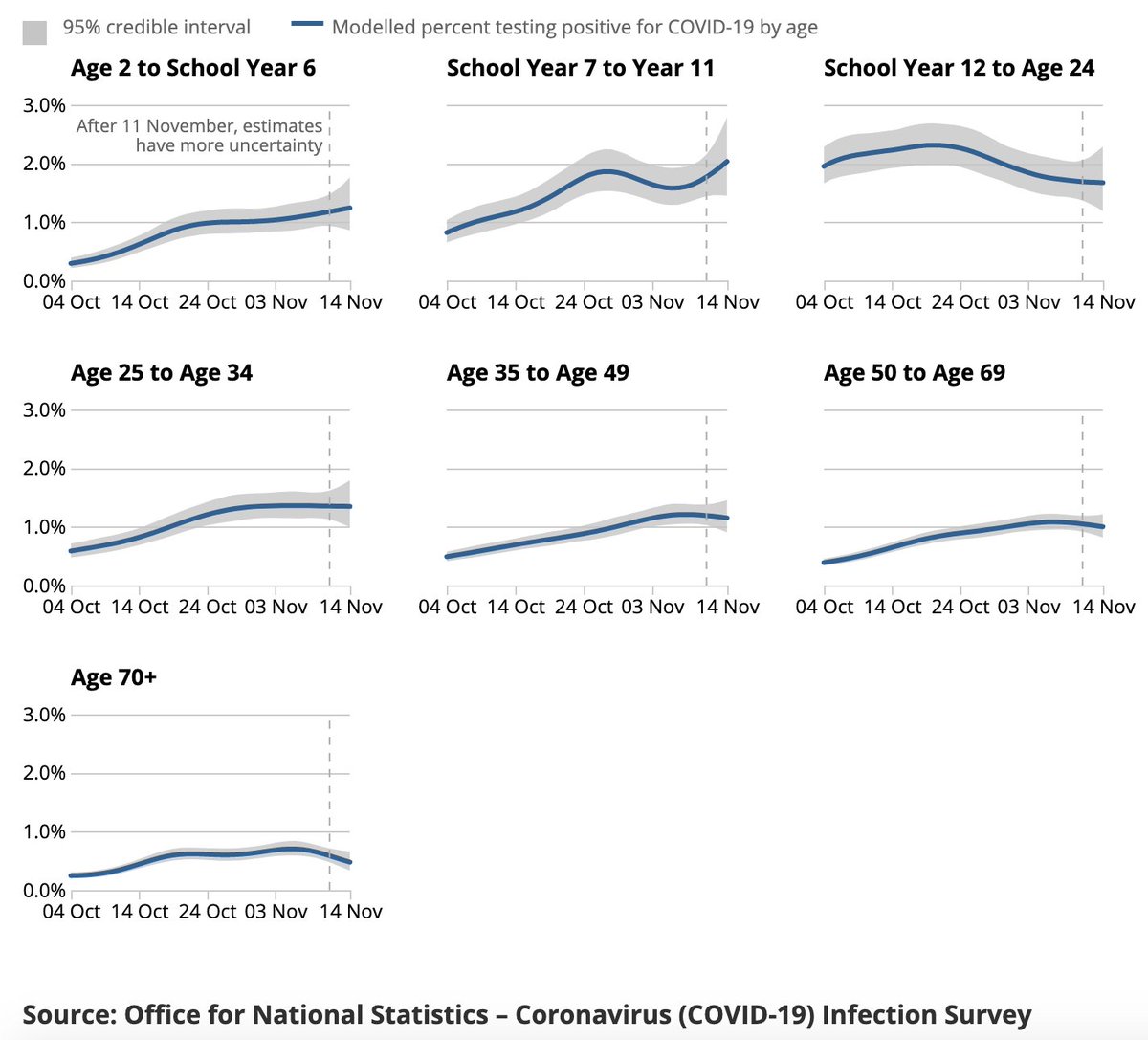
Looking at infection rates- ONS data suggest school children have similar or higher infection rates compared to adults, rising steeply since schools opened in September. Antibody studies show similar rates in older children relative to adults, & possibly lower in younger children 

It's important to remember that many of the studies on seroprevalence, and infection were carried out during a period where schools were either closed or attendance was low. There is also evidence that both viral PCR tests, and serology tests may be less sensitive in children.
Also symptom-based detection is unlikely to pick up cases in children because many are asymptomatic, or the symptoms are different from adults (and our symptom definitions for eligibility for testing for children have not been updated).
Do children transmit?
Yes. An earlier national study from S. Korea carried out when schools were closed showed that within household transmission was highest when the index case was 10-19 yrs old (19% of contacts infected), and lowest when the index was 0-9 yrs (5% of contacts)
Yes. An earlier national study from S. Korea carried out when schools were closed showed that within household transmission was highest when the index case was 10-19 yrs old (19% of contacts infected), and lowest when the index was 0-9 yrs (5% of contacts)
What does this mean in terms of school transmission?
It makes sense that even if children were somehow less likely to transmit at individual level, the much higher level of contacts within schools would easily make up for this. There is real-world evidence to support this
It makes sense that even if children were somehow less likely to transmit at individual level, the much higher level of contacts within schools would easily make up for this. There is real-world evidence to support this
We've had >1000 outbreaks of infection in schools in England since schools opened. A large proportion of outbreaks that occur within England are related to care home or educational settings. And both primary and secondary schools are the biggest contributors - in equal share.

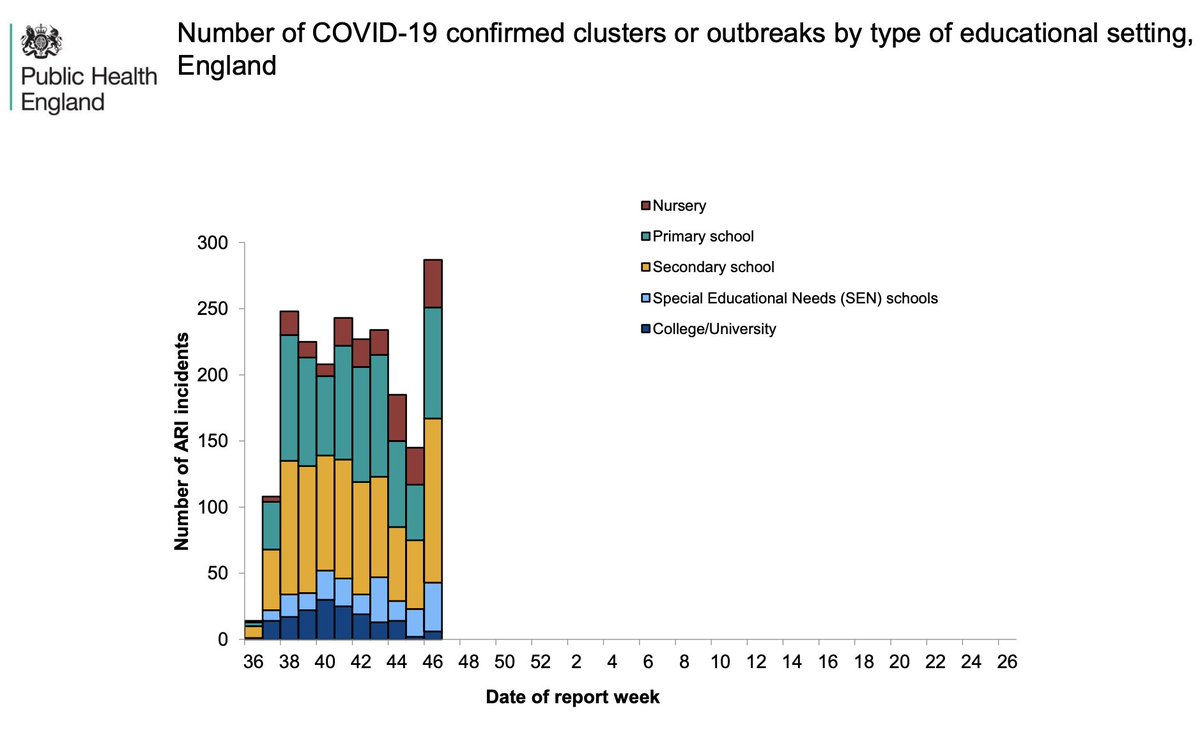
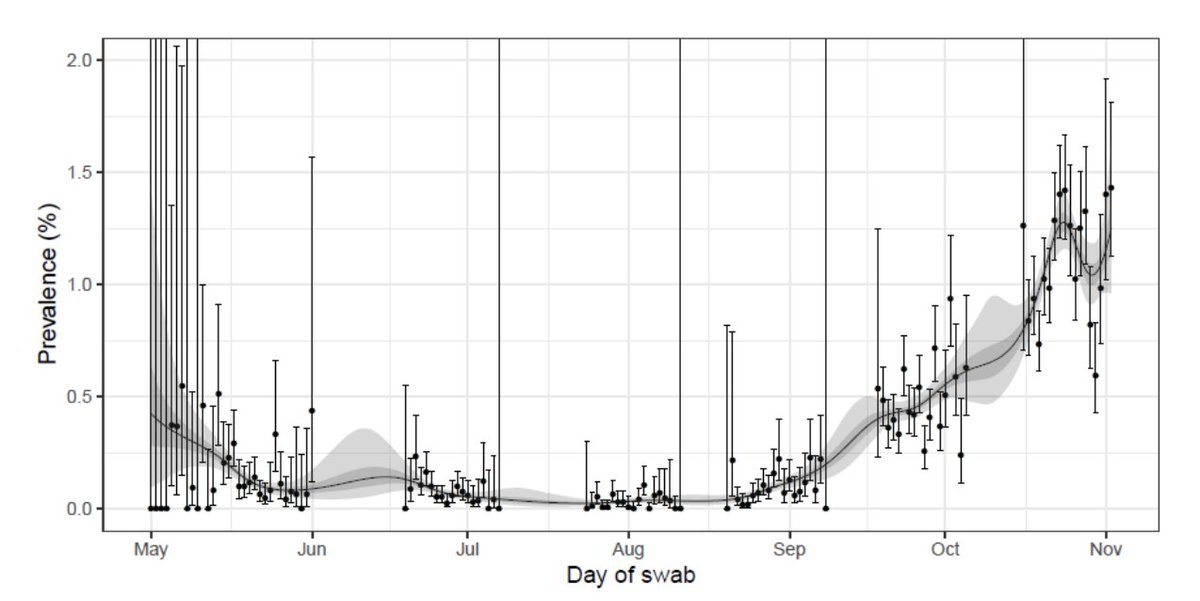
These outbreaks (in the previous tweet), and national trends of data from the ONS, and the REACT-1 study all suggest a reduction in outbreaks, and in overall cases during half-term, with a resumption in increase afterwards - continuing through lockdown
https://twitter.com/dgurdasani1/status/1329817757806948377?s=20
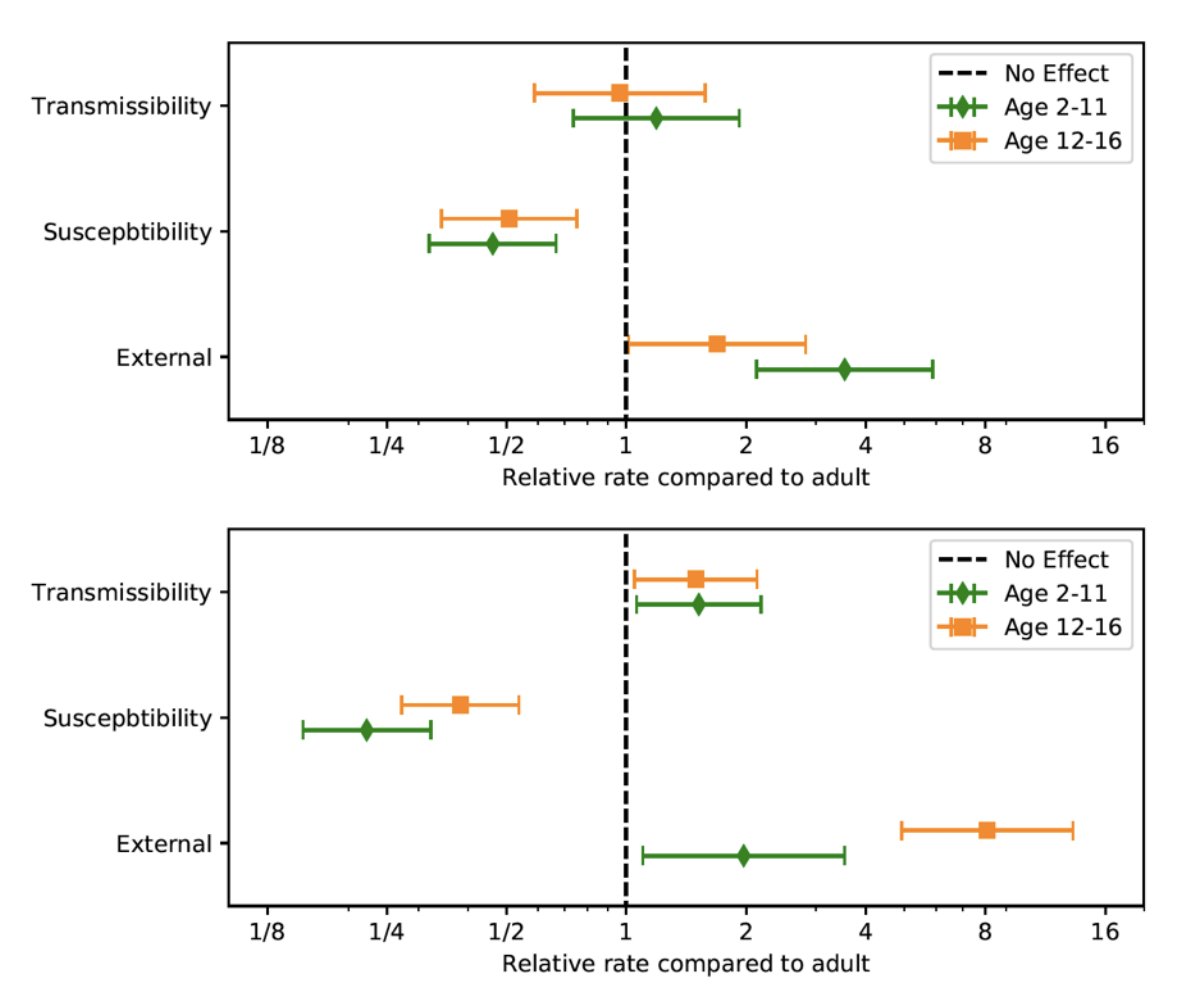
SAGE analysis of data from households suggest that secondary age school children are *8* times more likely than adults to bring infection into households & younger children *3* times more likely to bring in infection since schools opened in September (figs before and after sept)
What does global evidence show?
School closures statewide in the US were associated with *60%* reduction in daily cases, and deaths in one study.
jamanetwork.com/journals/jama/…
School closures statewide in the US were associated with *60%* reduction in daily cases, and deaths in one study.
jamanetwork.com/journals/jama/…
Recent evidence published suggests that educational institution closures in the second highest ranked intervention in terms of reducing transmission in an analysis of >200 countries.
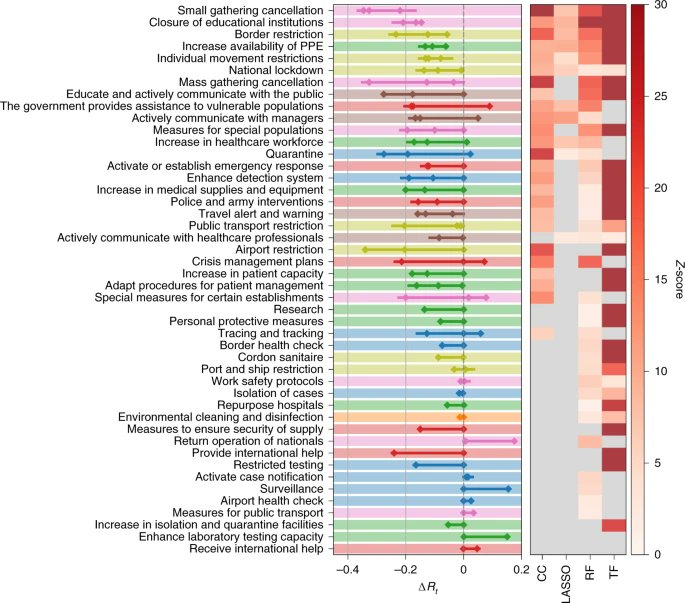
Breaking the data down, the effect is comparable across all educational institutions - pre-school, primary and secondary schools. The thinking that younger children don't contribute to transmission appears to be flawed.

But what about all those studies that suggested children don't contribute much to transmission?
Most of those studies were severely limited in that they were carried out during lockdown when schools were closed, or attendance was minimal. Background transmission also matters.
Most of those studies were severely limited in that they were carried out during lockdown when schools were closed, or attendance was minimal. Background transmission also matters.
Children are more likely to be asymptomatic so symptom-based testing often misses children & wrongly assigns the cause of infection to adults around them who are more likely to be symptomatic. Asymptomatic mass testing in schools has revealed many more cases in children when done
The evidence seems to be quite strong that school-age children- both primary and secondary contribute to transmission within schools, and across communities.
So why haven't we addressed this, despite accruing evidence that all points in this direction?
So why haven't we addressed this, despite accruing evidence that all points in this direction?
There seems to be a false dichotomy between keeping schools open with unmitigated spread, and closing schools down compromising children's education. These are certainly not the only options. There is so much more we can do to make schools safer for children, staff & communities.
This means investing in infrastructure, staff and protective equipment- including mask use in schools - primary and secondary, investment in ventilation, air filtration (as Germany is doing), using empty spaces for larger classrooms, smaller class sizes & more staff.
We also need to make arrangements and support schools and families with blended teaching or remote teaching for short periods of time, when absolutely necessary. This means provision of relevant infrastructure and training to teachers, and students, and provision of broadband.
And financial and practical support for family members who need to stay home to be with children if the need arises. As well as provision of free school meals at home. This has been done successfully in many countries, and can be done in England.
We also need better ways to detect outbreaks in school early on. The current system isn't working. Only children who develop symptoms get tested. It takes ~4-5 days to get results, while other children who are exposed remain in school.
Current guidelines only require those who have been in 'close contact' - within 2 m for >15 minutes to isolate. Often only children with desks around the infected child are required to isolate. This is out of step with evidence on airborne transmission in poorly vent settings.
We need asymptomatic screening to really control outbreaks in these settings, or at the very least, rapid testing turnaround, and isolation of the entire bubble or class.
There need to be clear guidelines in place for protection of vulnerable staff members, and households with vulnerable individuals living with children, so as to minimise the risk to them.
Current evidence looking at comparisons of infection rates of teachers with other workers is very flawed. There is a lot of uncertainty around estimates, & if anything the data appear to suggest that teachers in all contexts are at similar risk to other public-facing key workers.
Evidence from the recent OpenSAFELY that suggests that COVID-19 outcomes in parents of school age children are comparable to those in similar age groups without children has been used by some to suggest children don't really impact outcomes in parents. This is a very flawed study
For example, results from the study show that after correcting for factors in the study, non-COVID-19 deaths are much lower in parents than non-parents. This suggests that these groups are intrinsically not comparable, as deaths are overall lower in parents for other reasons.
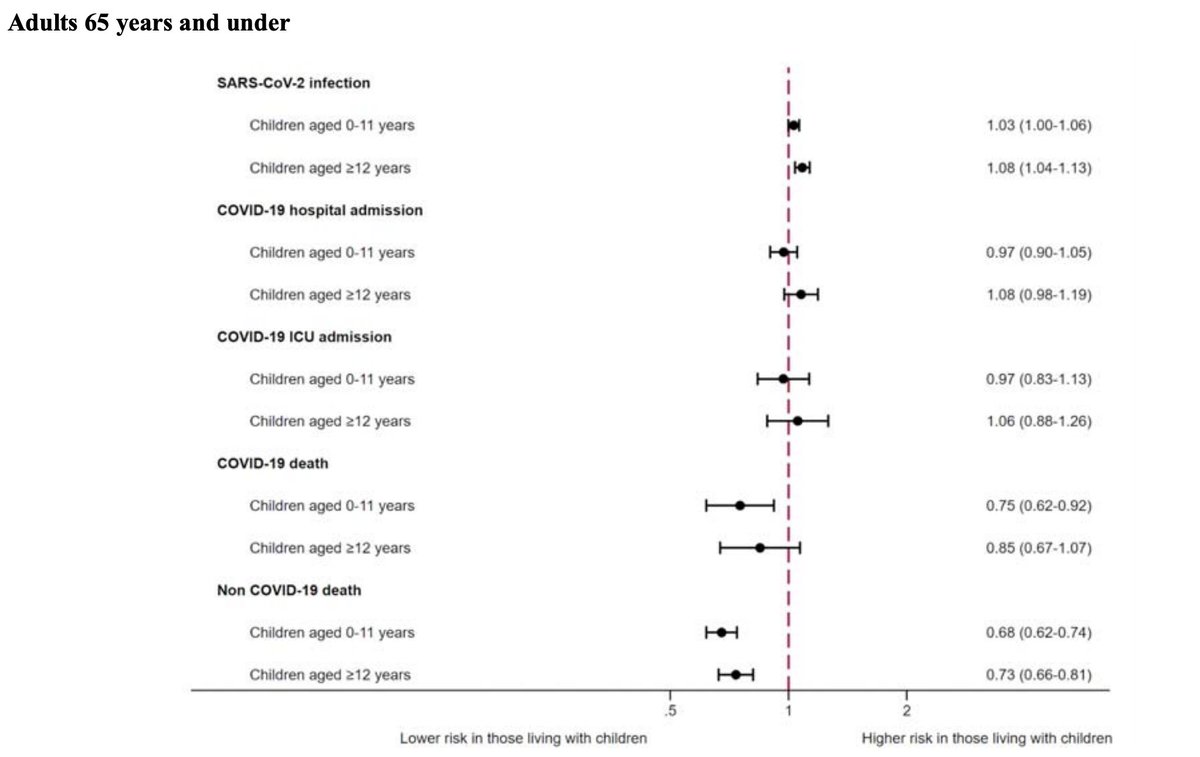
This means that health behaviours or other factors that have not been accounted for in the study are driving many of the outcomes. In fact, the study shows that parents of school children are more likely to be infected than non-parents, despite these groups not being comparable.
It's time to stop denying the overwhelming evidence that points to children playing an important role in transmission. Until we acknowledge this evidence, we will not be able to protect our children, staff, and communities. We need to translate this evidence into policy.
While a lot of current policy is based on the fact that COVID is less severe in children, there is more & more evidence emerging about multi-inflammatory syndromes & long COVID in children. This is a new disease we don't know a lot about. Is it fair to expose children to risk?
Ultimately, if we want to protect children's education, the best way to do this is minimise background transmission in the community, and put in place mitigatory measures in schools.
At the moment absenteeism due to COVID-19 is increasing in schools - 600K children were absent for COVID-19 related reasons last week. The current system isn't working. We need to do better.
• • •
Missing some Tweet in this thread? You can try to
force a refresh