Catching up on #burns patients on the #PedsICU - first up Steven E. Wolf discussing specialised burns care by the surgical team
He starts by discussing the ultimate goals of paediatric burn care:
- no deaths
- no scars
- no pain
We are improving but not there yet
#WFPICCS20
He starts by discussing the ultimate goals of paediatric burn care:
- no deaths
- no scars
- no pain
We are improving but not there yet
#WFPICCS20
‘Burns are as bad as they are going to get at the start; they can only get better - burns are different to chronic diseases’ - Steven E. Wolf, burns surgeon/Intensivist
#PedsICU #WFPICCS20
#PedsICU #WFPICCS20
What are the strategies for management of the #burn wound?
The key is fix and heal the wound. Then de-intensify the patient as soon as possible.
Remember: #burns wounds will have organisms cultured - but are they causing infection?
#PedsICU #WFPICCS
The key is fix and heal the wound. Then de-intensify the patient as soon as possible.
Remember: #burns wounds will have organisms cultured - but are they causing infection?
#PedsICU #WFPICCS

Surgical decision making in burns contains lots of complexity and is often a staged procedure: as a rule of thumb it’s 1 operation per 10% burn surface area
The aim is to get the wound closed as this reduces additional complications
#PedsICU #WFPICCS20 #Burns
The aim is to get the wound closed as this reduces additional complications
#PedsICU #WFPICCS20 #Burns

#Burns #resuscitation issues include:
- airway obstruction
- need for lots of volume (but this leads to its own set of complications!)
- compartment syndromes
- lung injury (from burns, smoke inhalation & fluid volume)
- need for renal support
#PedsICU #WFPICCS20
- airway obstruction
- need for lots of volume (but this leads to its own set of complications!)
- compartment syndromes
- lung injury (from burns, smoke inhalation & fluid volume)
- need for renal support
#PedsICU #WFPICCS20
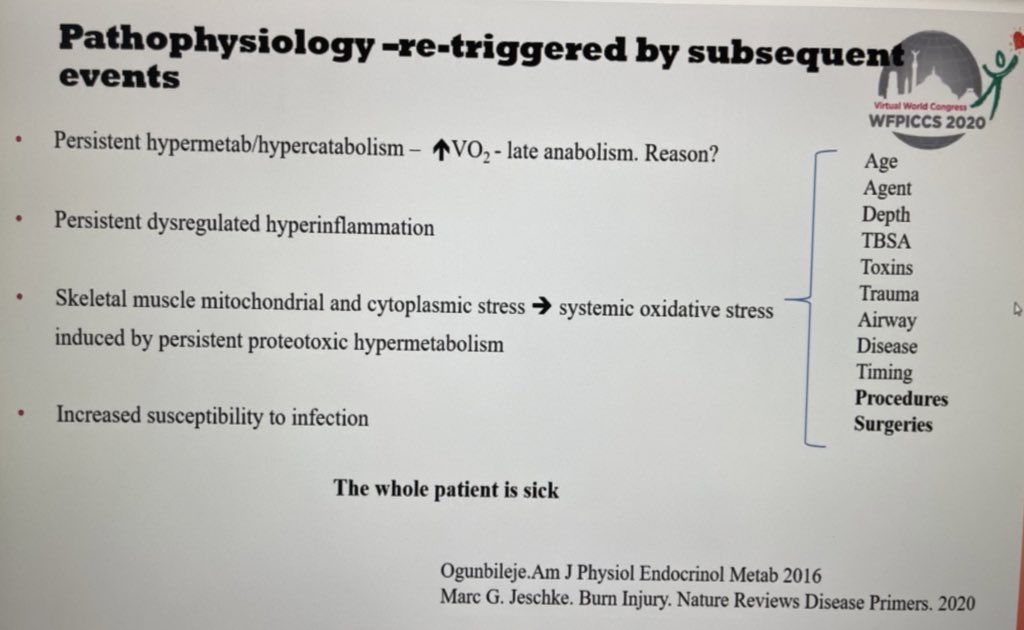
Longer term #burns issues on #PedsICU include:
- need to manage nutrition
- mobilise early
- Psychological support
Don’t forget delayed development of #sepsis from the burn wound!
#WFPICCS20
- need to manage nutrition
- mobilise early
- Psychological support
Don’t forget delayed development of #sepsis from the burn wound!
#WFPICCS20

Steven Wolf now tells us that in #burns looking for signs of #sepsis can be hard - there is no correlation with temperature and white cell count in these children
Low index of suspicion.
#PedsICU #WFPICCS20
Low index of suspicion.
#PedsICU #WFPICCS20

• • •
Missing some Tweet in this thread? You can try to
force a refresh