Still waiting on that contact tracing data for KC restaurants and bars. What % of outbreaks can you trace to them? Why haven't you shared this when you have 9 months of data?
A well-documented anecdote (3 infections) does not mean this is happening everywhere all the time.
A well-documented anecdote (3 infections) does not mean this is happening everywhere all the time.
https://twitter.com/QuintonLucasKC/status/1338834982073196545
"Necessary curbs", @QuintonLucasKC says, but provides no specifics, no data for Kansas City to show why this is necessary. These are the actions of someone desperate to look like he's doing something even if it's not empirically driven.
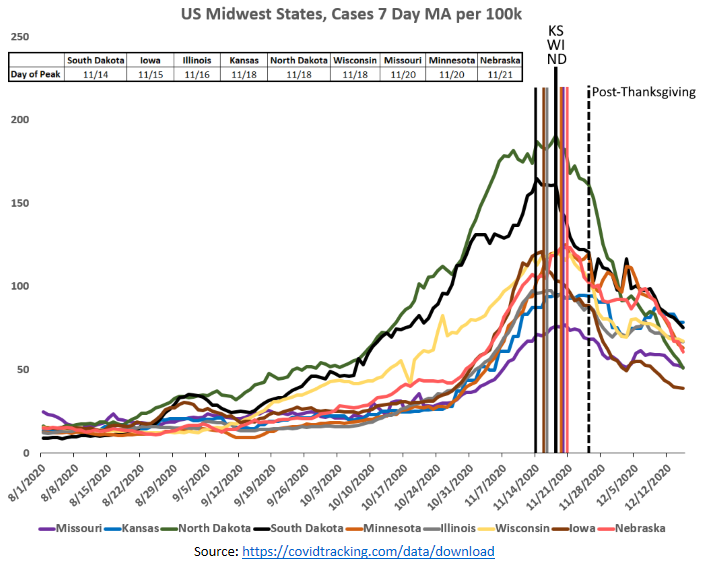
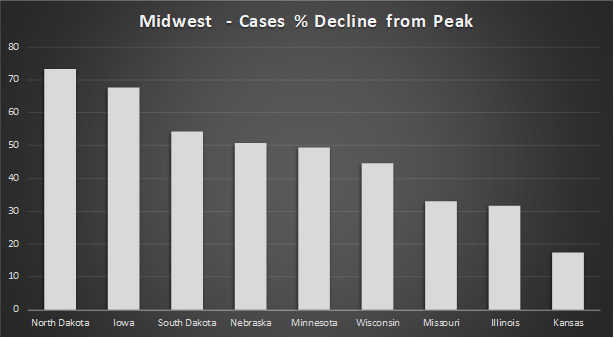
Also, cases are decreasing in KC as they are throughout the rest of the Midwest. @QuintonLucasKC announced his "Safer at Home KC" measures on 11/16. Cases peaked around 11/10. His policies are so effective they work retroactively! 

The funny thing is, the other day Lucas was asked how many cases could be traced to bars in Kansas City and his answer was "40% of recent cases in Kansas City are people in their 20s and 30s". That......doesn't answer the question.
https://twitter.com/FactsVs0pinion/status/1338164615499354113?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh