The WHO’s chief scientist on a year of loss and learning nature.com/articles/d4158…
For anyone remotely involved in healthcare, these are life lessons from @doctorsoumya. A must read.
For those of you who want a quick analysis, thread.
For anyone remotely involved in healthcare, these are life lessons from @doctorsoumya. A must read.
For those of you who want a quick analysis, thread.
Disclaimer: I’m just breaking this up & annotating them with my own comments. Between quotes are her exact words (with some poetic license) 

Planning ahead & prioritizing first steps – an important aspect of taking up a new job
“My original plan for 2020 included rolling out new processes to ensure the quality of technical documents, such as guidelines on water quality, tobacco advertising and immunization programmes”
“My original plan for 2020 included rolling out new processes to ensure the quality of technical documents, such as guidelines on water quality, tobacco advertising and immunization programmes”
The ability and sheer necessity of changing plans at short notice – a necessary skill for handling the pandemic
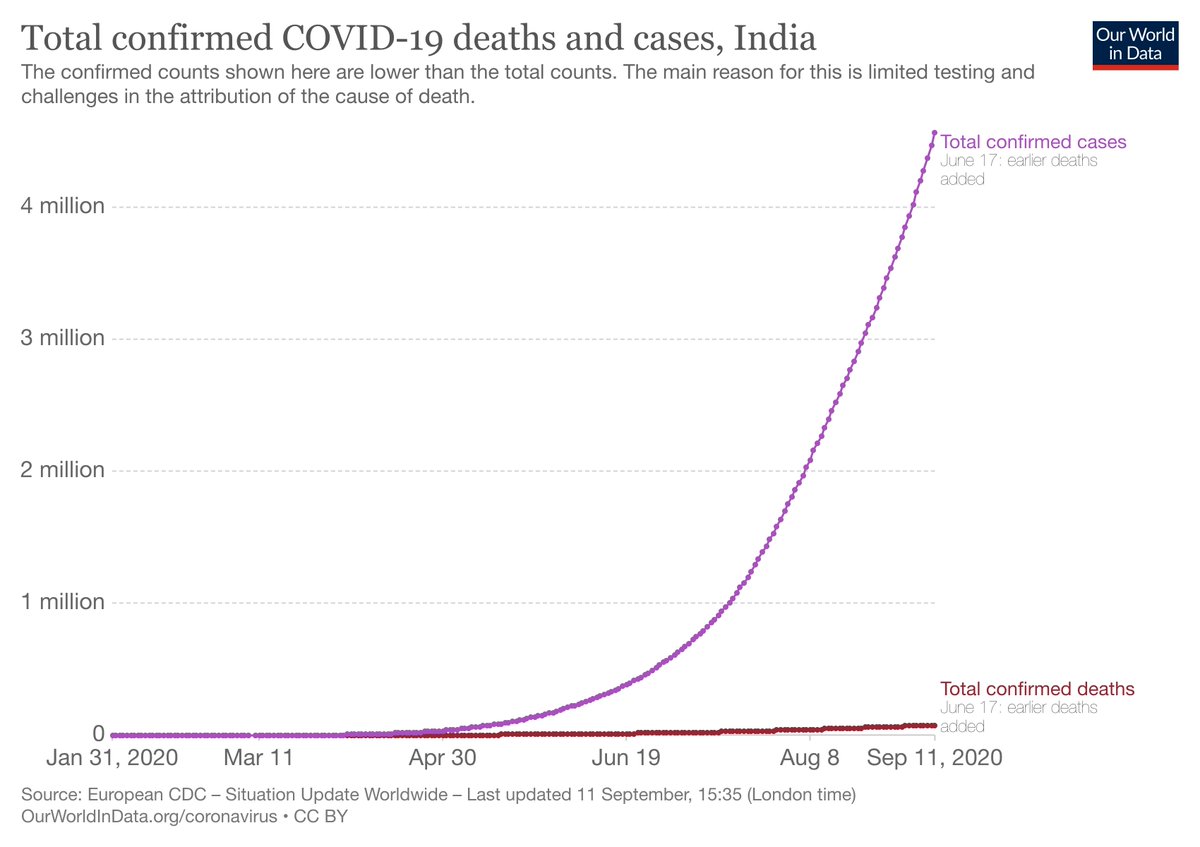
“All those plans changed on 31 Dec 2019. WHO was informed about a cluster of viral-pneumonia cases of unknown origin in Wuhan, China: the disease later named COVID-19”
“All those plans changed on 31 Dec 2019. WHO was informed about a cluster of viral-pneumonia cases of unknown origin in Wuhan, China: the disease later named COVID-19”
Two crucial attributes of a leader: Believe in and credit the team; Accept your own and your organization’s weaknesses.
“I am proud of many things my team has achieved in the past 12 months, even as the shortcomings of both the WHO and the global community have been laid bare”
“I am proud of many things my team has achieved in the past 12 months, even as the shortcomings of both the WHO and the global community have been laid bare”
Face challenges head-on
“We’ve had to balance speed & rigour. We’ve had to raise alarm without causing panic. We’ve had to convince countries without openly criticizing them (which would risk losing their cooperation). We’ve had to fight the ‘infodemic’, sticking to science”
“We’ve had to balance speed & rigour. We’ve had to raise alarm without causing panic. We’ve had to convince countries without openly criticizing them (which would risk losing their cooperation). We’ve had to fight the ‘infodemic’, sticking to science”
The cross leaders bear… the burden of responsibility
“Countries, especially low- and middle-income ones, depend on the WHO to decide how to combat disease and preserve public health”
“Countries, especially low- and middle-income ones, depend on the WHO to decide how to combat disease and preserve public health”
Learning from past mistakes, and having the courage to acknowledge them
“In 2007, following much (largely deserved) criticism of its procedures, such as not always basing decisions on evidence, the WHO set out rigorous, standardized procedures; transparency, evidence-base & COI”
“In 2007, following much (largely deserved) criticism of its procedures, such as not always basing decisions on evidence, the WHO set out rigorous, standardized procedures; transparency, evidence-base & COI”
Breaking convention to handle a crisis
“A typical WHO conference requires months to plan — it takes that long for visas to come through. We pulled it off with three weeks’ notice, finding ways to involve those who couldn’t travel”
“A typical WHO conference requires months to plan — it takes that long for visas to come through. We pulled it off with three weeks’ notice, finding ways to involve those who couldn’t travel”
The failure of much of scientific research – small, underpowered studies
“it quickly became apparent that we needed global coordination for clinical trials — some 2,000 were already under way, most of which were too small to be definitive”
“it quickly became apparent that we needed global coordination for clinical trials — some 2,000 were already under way, most of which were too small to be definitive”
When life serves you lemons, make lemonade…
“We launched prospective meta-analyses encouraging principal investigators running trials of corticosteroids for treatment of COVID-19 to collaborate and share data”
“We launched prospective meta-analyses encouraging principal investigators running trials of corticosteroids for treatment of COVID-19 to collaborate and share data”
The power of persuasion
“It contacted about a dozen researchers running clinical trials of the steroid dexamethasone, convinced them to share data even while the trials were ongoing
Normally, such guidelines take 6–12 months to produce; the committee has cut the time to 6 weeks”
“It contacted about a dozen researchers running clinical trials of the steroid dexamethasone, convinced them to share data even while the trials were ongoing
Normally, such guidelines take 6–12 months to produce; the committee has cut the time to 6 weeks”
The whole should be [and usually is larger (and better)] than the sum of its parts…
“This led to the WHO engaging more than 90 institutions in a new partnership; we set up advisory groups of global experts for more than 20 topics”
“This led to the WHO engaging more than 90 institutions in a new partnership; we set up advisory groups of global experts for more than 20 topics”
There is no need to monopolize the effort (and the credit); there’s plenty for us (and others) to do
“The Cochrane Collaboration has a similar initiative— there is more than enough of this work to do”
“The Cochrane Collaboration has a similar initiative— there is more than enough of this work to do”
Never waste a good crisis…
“The one thing I’m proudest of is the setting up of a multi-country, adaptive clinical trial to test multiple treatments at once. This format adds or removes trialled therapeutic agents as new data emerge, while continuing to recruit participants”
“The one thing I’m proudest of is the setting up of a multi-country, adaptive clinical trial to test multiple treatments at once. This format adds or removes trialled therapeutic agents as new data emerge, while continuing to recruit participants”
The humility to accept that “the slaying of a beautiful hypothesis by an ugly fact” is what science is about
“Interim results from 12,000 participants from 30 countries have been disappointing, with none of the tested drugs showing reductions in mortality or disease progression”
“Interim results from 12,000 participants from 30 countries have been disappointing, with none of the tested drugs showing reductions in mortality or disease progression”
Yet, look at the bright side of life.
“But the approach has shown how to perform high-quality randomized clinical trials to assess potential drugs and answer public-health questions even during a pandemic”
“But the approach has shown how to perform high-quality randomized clinical trials to assess potential drugs and answer public-health questions even during a pandemic”
The dangers of disinformation & fake news – an epidemic of the modern world
“Meanwhile, the WHO has been communicating evidence and debunking misinformation as never before. Launched in March, the WHO Health Alert chatbot counters false information”
“Meanwhile, the WHO has been communicating evidence and debunking misinformation as never before. Launched in March, the WHO Health Alert chatbot counters false information”
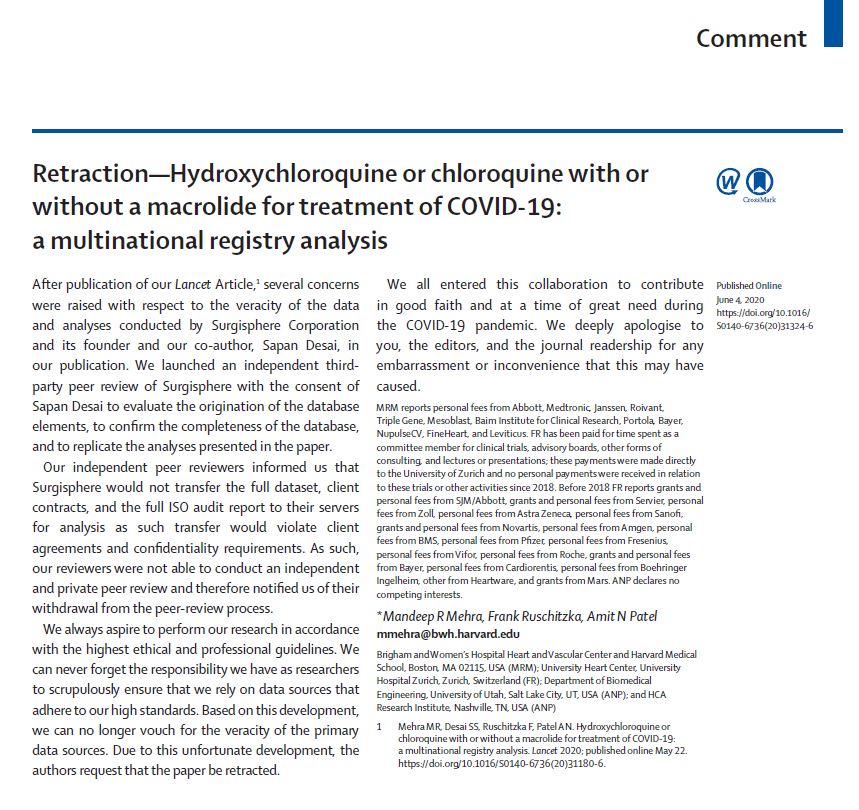
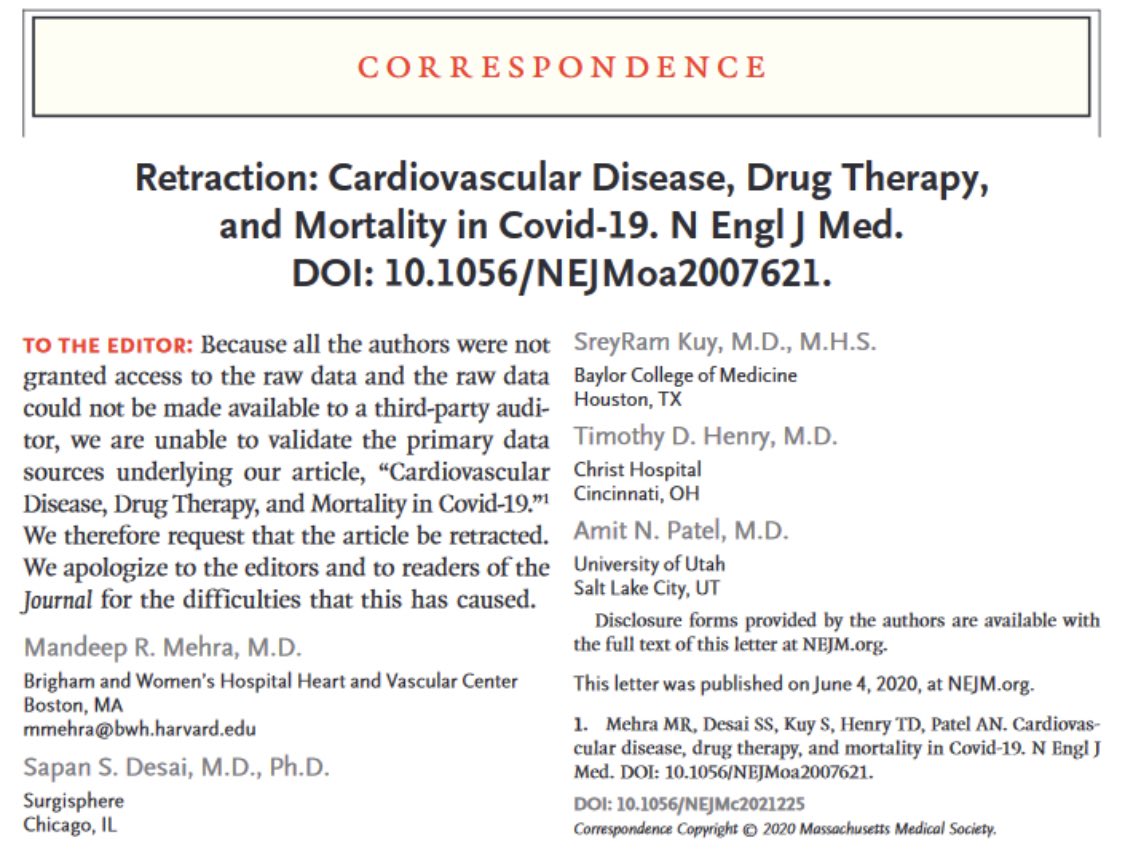
An underrated statement – why researchers should share data.
“We need a stronger infrastructure and culture of sharing.
Looking ahead, funders, institutions and other players need to create better mechanisms to reward researchers who share … data”
“We need a stronger infrastructure and culture of sharing.
Looking ahead, funders, institutions and other players need to create better mechanisms to reward researchers who share … data”
The importance of preparedness; and having a plan.
“As I have sought ways to make good decisions quickly, the lesson that repeats itself is how important it is to have thoughtful plans prepared and in place”
“As I have sought ways to make good decisions quickly, the lesson that repeats itself is how important it is to have thoughtful plans prepared and in place”
Paraphrasing @PeterASinger: Good leadership is the best vaccine
“The countries that have best protected the lives and livelihoods of their citizens have also demonstrated strong, compassionate leadership, at political and technical levels”
“The countries that have best protected the lives and livelihoods of their citizens have also demonstrated strong, compassionate leadership, at political and technical levels”
The real bottomline – no shortcuts to good healthcare systems and a culture of R&D.
“…have health-care systems that engage local and global communities. These qualities require long-standing investments in people and relationships, as well as in research and development”
“…have health-care systems that engage local and global communities. These qualities require long-standing investments in people and relationships, as well as in research and development”
The power (& need) for effective communication
“Not coincidentally, I have seen the value of listening & two-way communication. Scientists talk to each other, but too often leave others behind. Citizens want to know what the evidence is, including explaining gaps or mistakes” End
“Not coincidentally, I have seen the value of listening & two-way communication. Scientists talk to each other, but too often leave others behind. Citizens want to know what the evidence is, including explaining gaps or mistakes” End
• • •
Missing some Tweet in this thread? You can try to
force a refresh