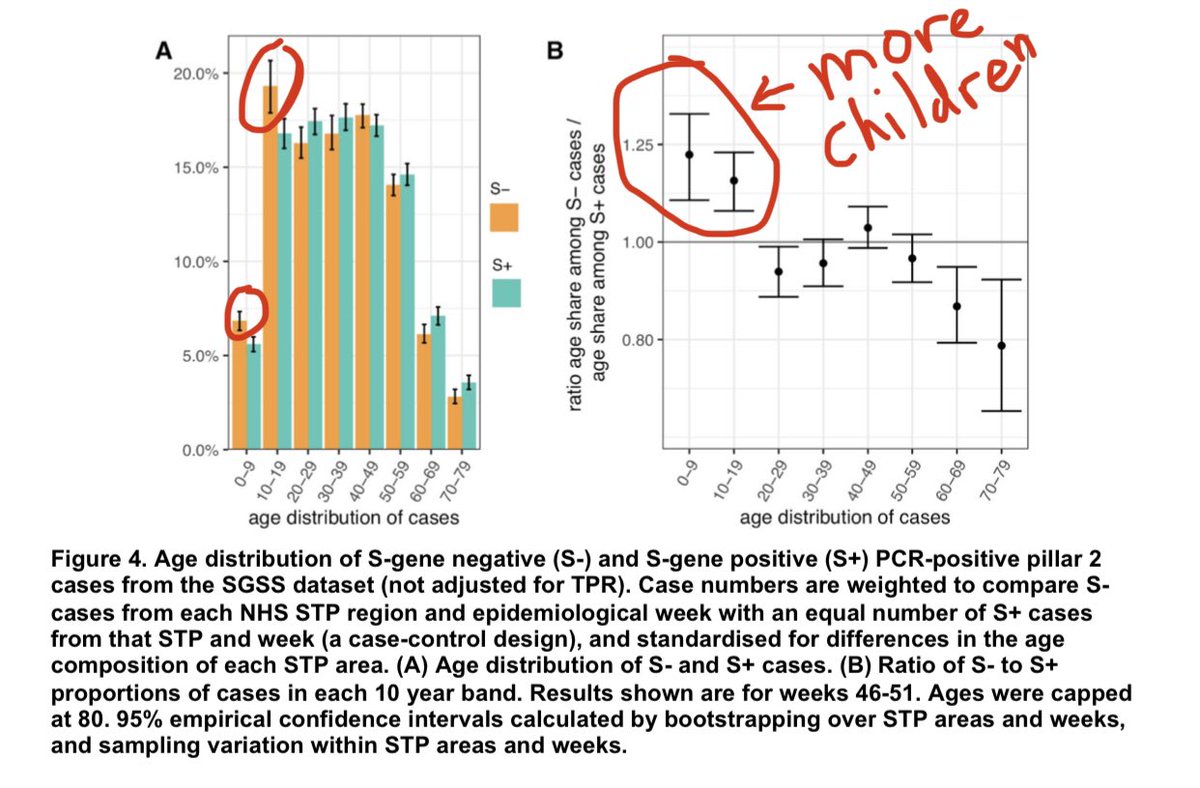
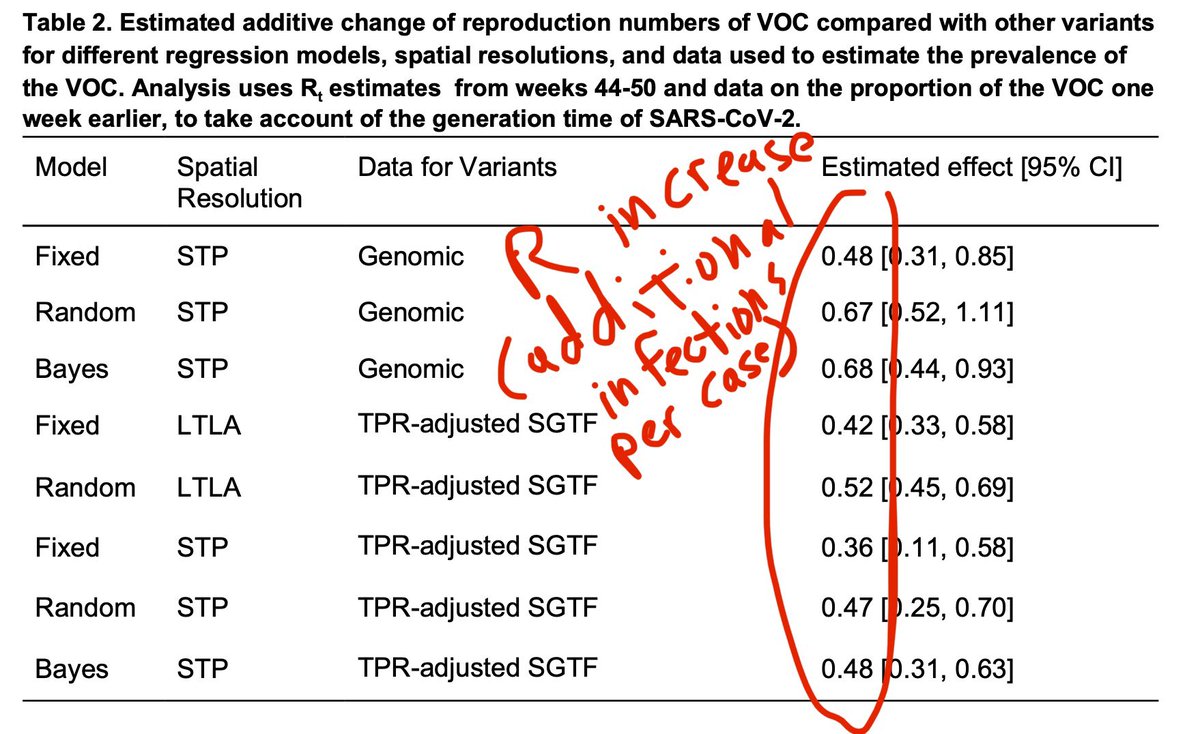
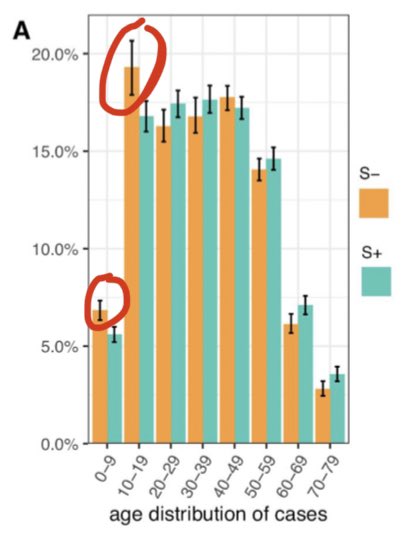
📍Worrisome new data—new B117 variant is not only more infectious, it’s potentially more infectious in children 0-9 (+24%) and 10-19 (+14%), and less among 60-79, compared to common strains. More sobering—the R estimate is much higher.
THREAD🧵 #COVID19 imperial.ac.uk/media/imperial…
THREAD🧵 #COVID19 imperial.ac.uk/media/imperial…
2) For R, various estimates range from 0.36 to 0.68 (higher R via more accurate sequenced virus samples, lower R estimate via shortcut PCR test w/ more data). This means every person infected w/ B.1.1.7 variant **infects additional +0.36 to +0.68 persons** than old strain. Wow.
3) To be clear, the graph shows the relative proportion of each age group for the B117 strain versus the *same age group* of the other strain, adjusted for geography & week. Thus its not just “school open” effect. It’s versus the common strain’s same age group, adjusted for time.

4) Given this evidence, I think we need to rethink school reopenings until we get this new B117 variant strain under control. We need every teacher and school worker (bus drivers, cafeteria staff, custodians) vaccinated before we got back to school. It pains me to say it though.
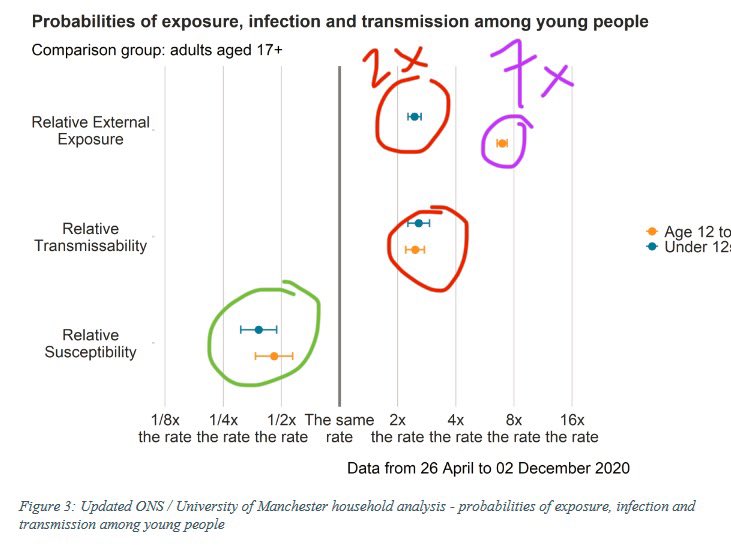
5) To be clear, there is a concern there is a school effect, but the Imperial team adjusted for time (what week it was). And this isn’t saying kids are more infectious than adults—likely now on par with adults (kids were lower risk with older strain).
6) if schools were open, then shouldn’t common strain also infect a lot more kids during the school-open-weeks too w/ equal opportunity? And again, adjusted for week timing effect.
Again, kids not higher risk than adults. But question is new vs old strains for kids of same age.
Again, kids not higher risk than adults. But question is new vs old strains for kids of same age.
7) Let me rephrase here—if you passionate believe it’s school-open effect alone, with more kids exposed—then think hard—shouldn’t the other common strains have **equal opportunity to infect** and be on par with new B117 strain if all strains are equal in transmission potential?
8) But that is not the case here. When given the chance to infect more kids, the variant dominated within each age group. But it didn’t dominate among adults as much.
9) Someone else said, “oh the data is old in Nov during the first lockdown”. Not entirely—data came from 2020 weeks 46-51 which spans mid Nov to mid Dec. 🇬🇧softer lockdown was Nov-Dec 2nd, harder lockdown was after Dec 19th. So adults were not lockdown (soft or hard) Dec 2-18th.
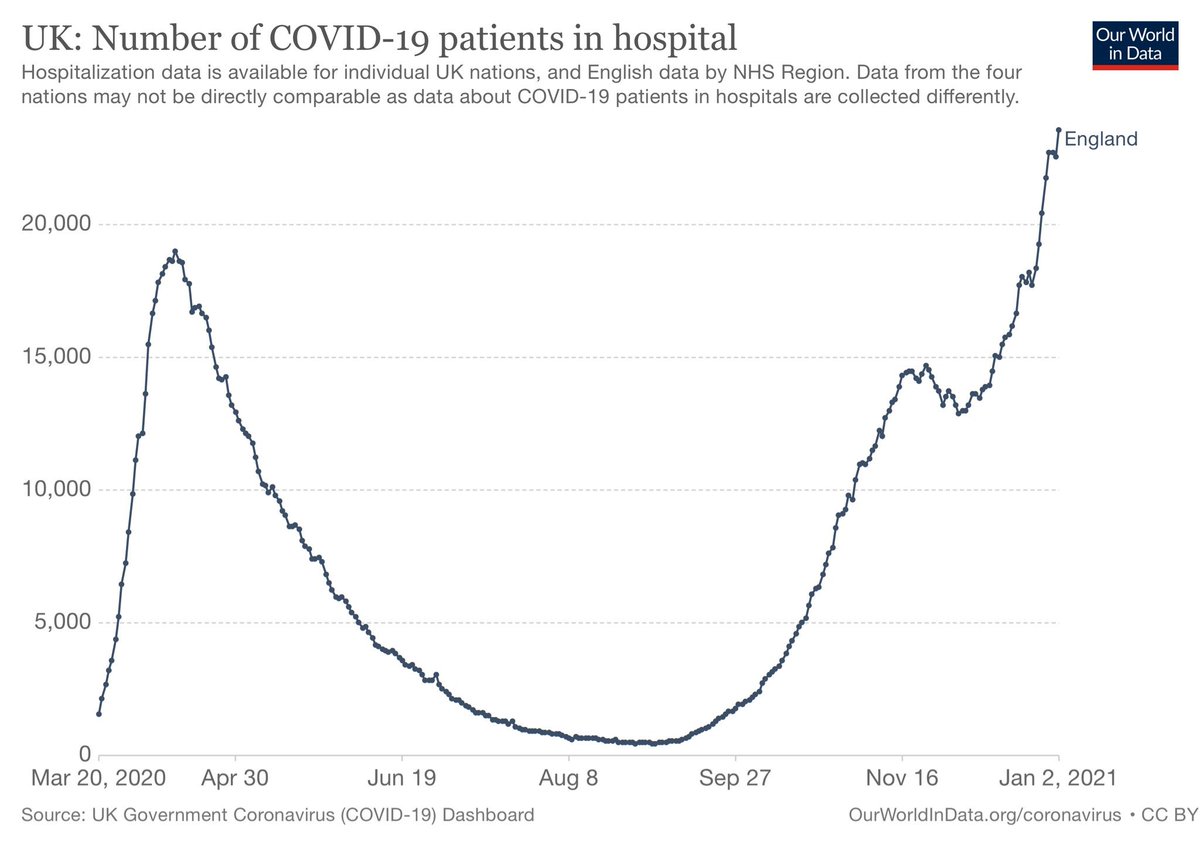
10) Latest hospital admissions data in England 🏴 — children 5 years old and under is surging. Children 6-17 also elevated. And the pediatric hospitalization curves are increasing faster than adults. Maybe school reopening effect, but kids 0-5 are typically not in formal schools.
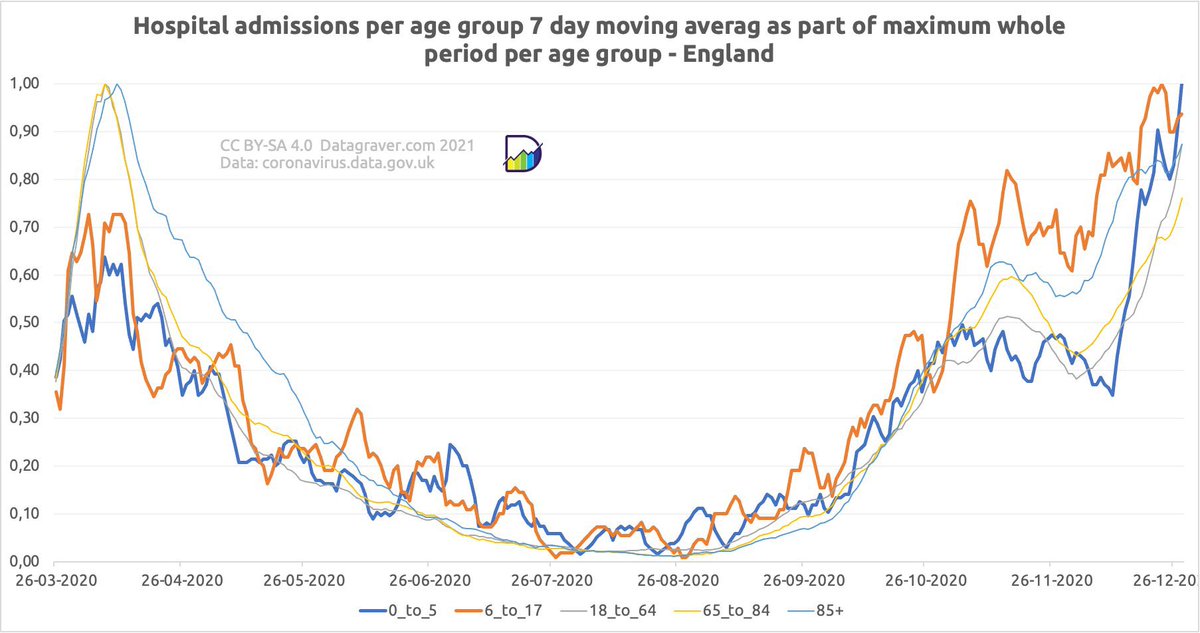
11) here is the link to the UK data for England hospitalizations by age above^. HT to @Datagraver for the graph and @adamhamdy for the referral to the data. Data transparency is just as key.
Correction - England (not all of UK) did have a tier 3 restriction from Dec 2nd.

12) To be clear, I did not say it’s precisely “24% more infectious”. I’m saying it could be more infectious—here look at 24% higher numbers [incidence].”
Other experts indeed acknowledge it may turn out to be more infectious in children. Let’s look for more confirmation.
Other experts indeed acknowledge it may turn out to be more infectious in children. Let’s look for more confirmation.
• • •
Missing some Tweet in this thread? You can try to
force a refresh