(1/6) It may seem hard to believe, but Western Australia has recorded no community transmission of COVID-19 since April 2020.
How? A lockdown to eliminate the virus, followed by border controls and quarantine to keep it out.
#ZeroCOVID is possible.
abc.net.au/news/2021-01-1…
How? A lockdown to eliminate the virus, followed by border controls and quarantine to keep it out.
#ZeroCOVID is possible.
abc.net.au/news/2021-01-1…
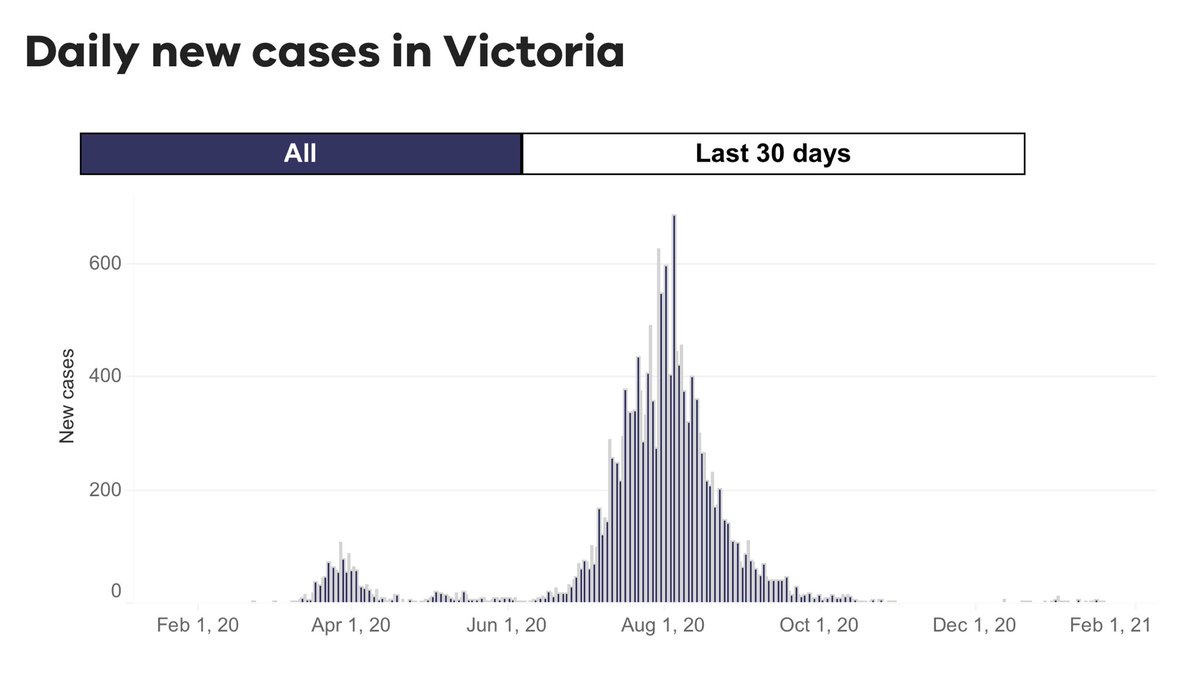
(2/6) But Australia’s an island, I hear you say. That’s true, and it certainly makes elimination easier. However, Australia had major outbreaks elsewhere.
The state of Victoria has recorded 20,433 cases & 820 deaths, mostly during a second wave in August.
dhhs.vic.gov.au/victorian-coro…
The state of Victoria has recorded 20,433 cases & 820 deaths, mostly during a second wave in August.
dhhs.vic.gov.au/victorian-coro…
(3/6) If unchecked, these outbreaks would have spread to the entire country. They didn’t because of internal border controls. Travel within Australia was restricted.
There is no reason why a similar red zone/green zone strategy couldn’t be implemented elsewhere. e.g., in Europe.
There is no reason why a similar red zone/green zone strategy couldn’t be implemented elsewhere. e.g., in Europe.
(4/6) Although severe, the epidemics in Europe, Canada, and even South America or the US could still be brought under control if the right measures were taken.
This article describes how the Australian state of Victoria beat their second wave.
This article describes how the Australian state of Victoria beat their second wave.
https://twitter.com/drzoehyde/status/1342511778387828736?s=21
(5/6) Of course, there is no certainty that an elimination strategy will be successful.
However, even if you fail, aiming for elimination guarantees a better outcome than if you aim for a lesser goal.
However, even if you fail, aiming for elimination guarantees a better outcome than if you aim for a lesser goal.
https://twitter.com/drzoehyde/status/1339172996645150725?s=21
(6/6) It’s not too late to aim for #ZeroCOVID.
https://twitter.com/drzoehyde/status/1342834794716020737?s=21
• • •
Missing some Tweet in this thread? You can try to
force a refresh