1/14
Why is cerebrospinal fluid (CSF) glucose low in bacterial meningitis?
Before we review potential mechanisms, I'm interested in the explanation you've heard/used.
What do you think causes low CSF glucose (hypoglycorrhachia)?
Why is cerebrospinal fluid (CSF) glucose low in bacterial meningitis?
Before we review potential mechanisms, I'm interested in the explanation you've heard/used.
What do you think causes low CSF glucose (hypoglycorrhachia)?
2/
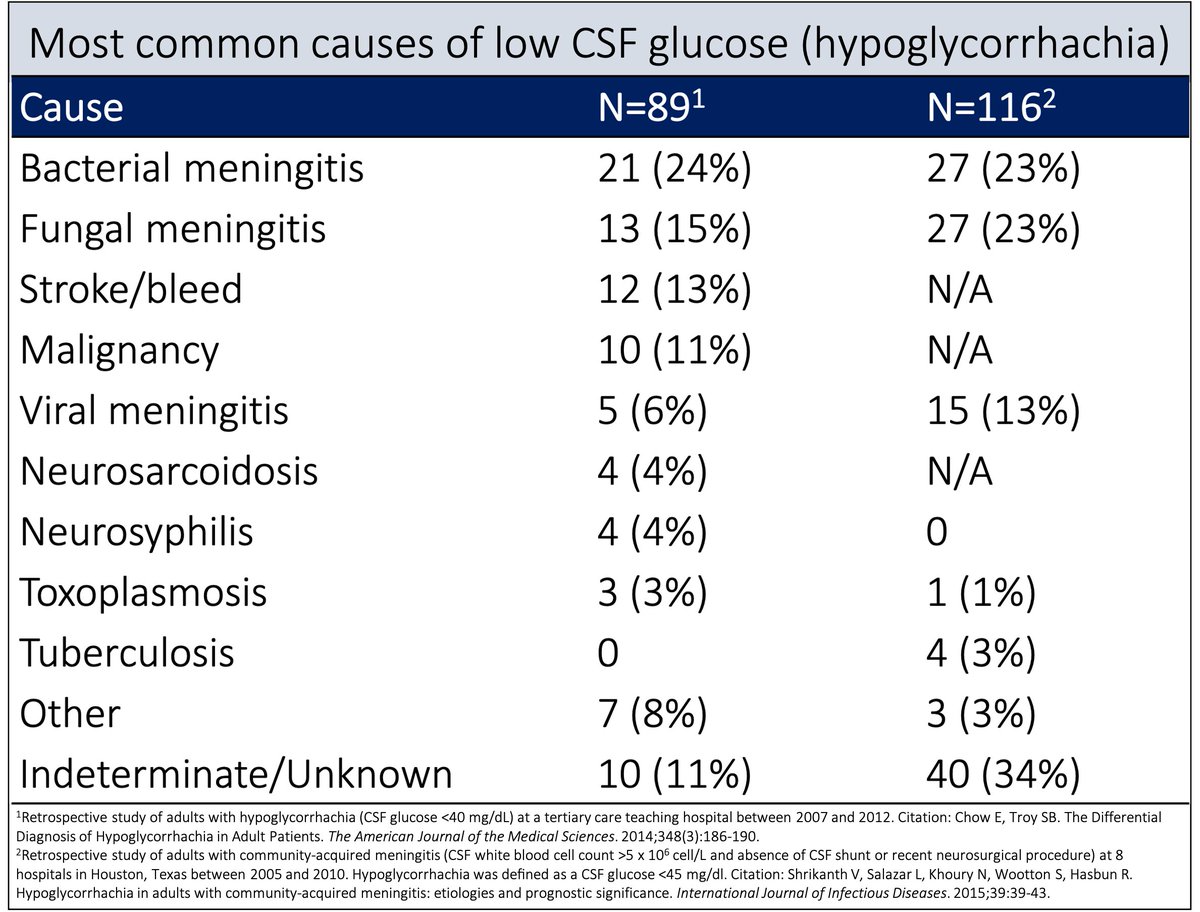
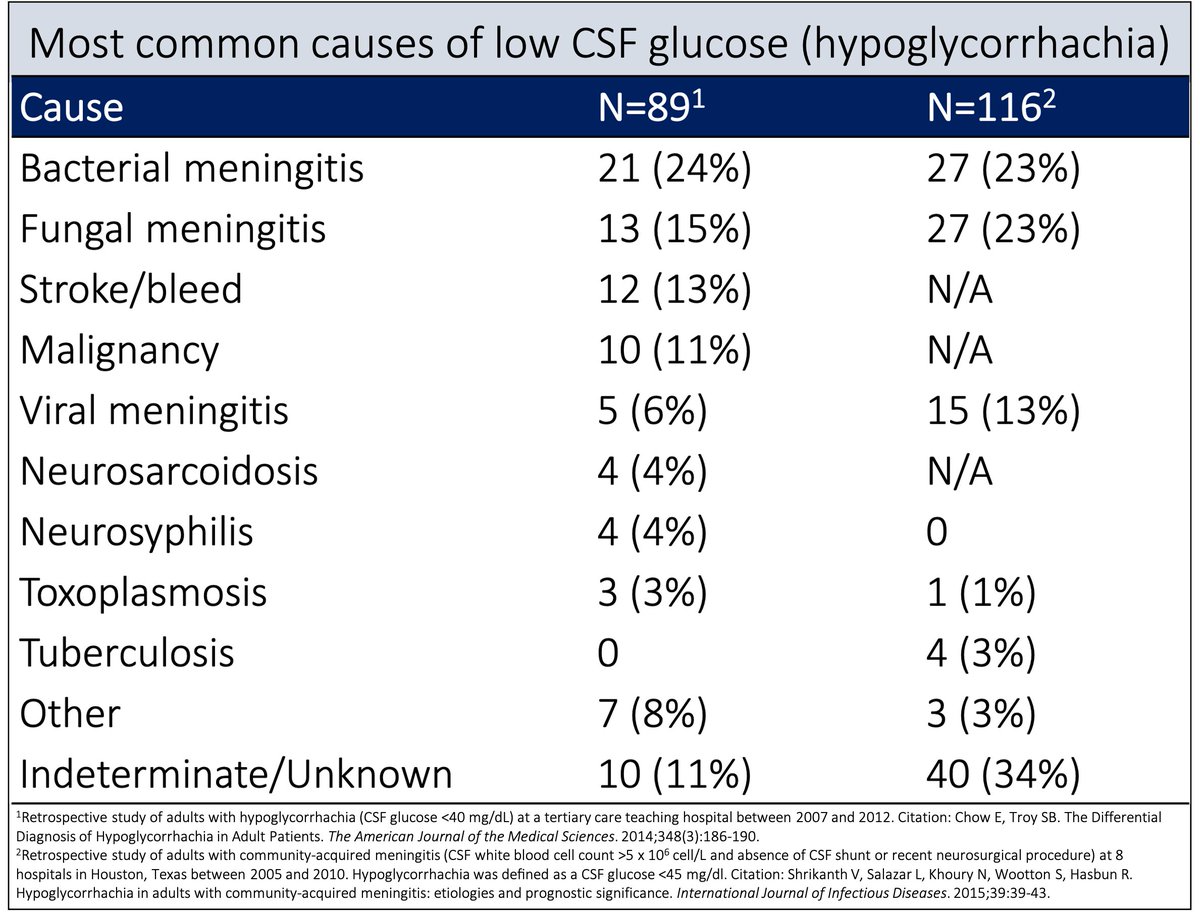
First, let's examine the most common causes of hypoglycorrhachia.
☞ While bacterial meningitis is the single most common cause, it accounts for fewer than a quarter of cases.
We'll come back to this.
pubmed.ncbi.nlm.nih.gov/24326618/
pubmed.ncbi.nlm.nih.gov/26299186/
First, let's examine the most common causes of hypoglycorrhachia.
☞ While bacterial meningitis is the single most common cause, it accounts for fewer than a quarter of cases.
We'll come back to this.
pubmed.ncbi.nlm.nih.gov/24326618/
pubmed.ncbi.nlm.nih.gov/26299186/
3/
Now to the potential mechanisms. A number of hypotheses have been offered to explain hypoglycorrhachia.
🔹Bacterial consumption of glucose
🔹WBC consumption
🔹Brain consumption
🔹Decreased entry into CSF
...and others
Let's examine these.
Now to the potential mechanisms. A number of hypotheses have been offered to explain hypoglycorrhachia.
🔹Bacterial consumption of glucose
🔹WBC consumption
🔹Brain consumption
🔹Decreased entry into CSF
...and others
Let's examine these.
4/
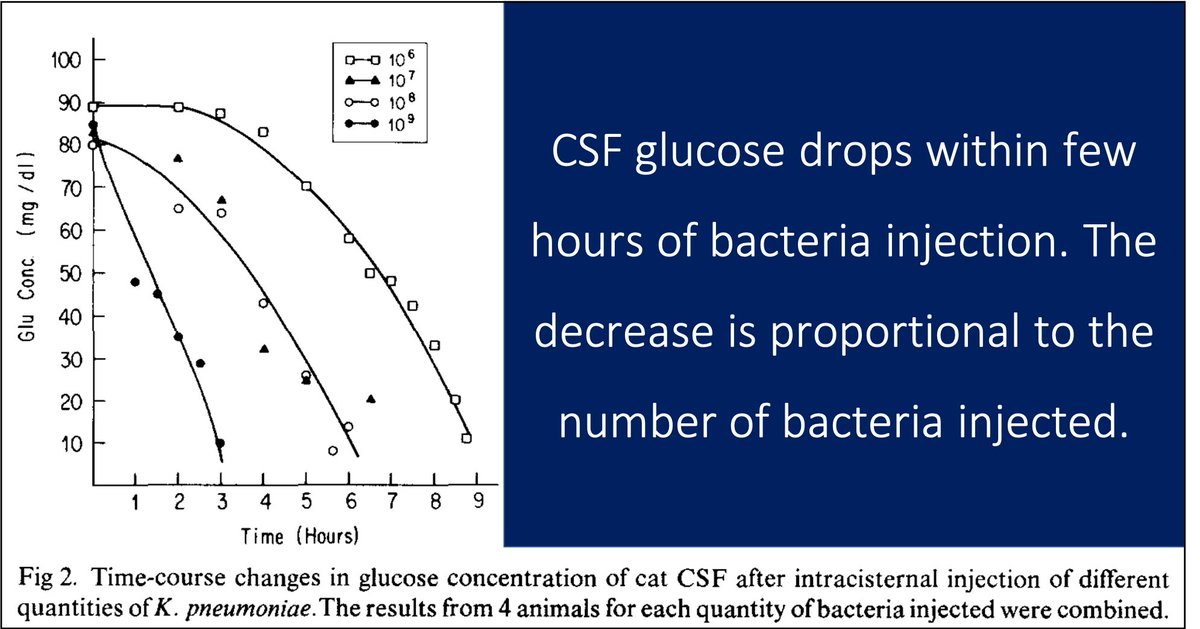
One of the first hypotheses offered was that the pathogenic bacteria consume glucose.
There are some experimental data supporting this. One study found that injection of bacteria into the CSF decreased glucose within a few hours.
pubmed.ncbi.nlm.nih.gov/6374041/
One of the first hypotheses offered was that the pathogenic bacteria consume glucose.
There are some experimental data supporting this. One study found that injection of bacteria into the CSF decreased glucose within a few hours.
pubmed.ncbi.nlm.nih.gov/6374041/
5/
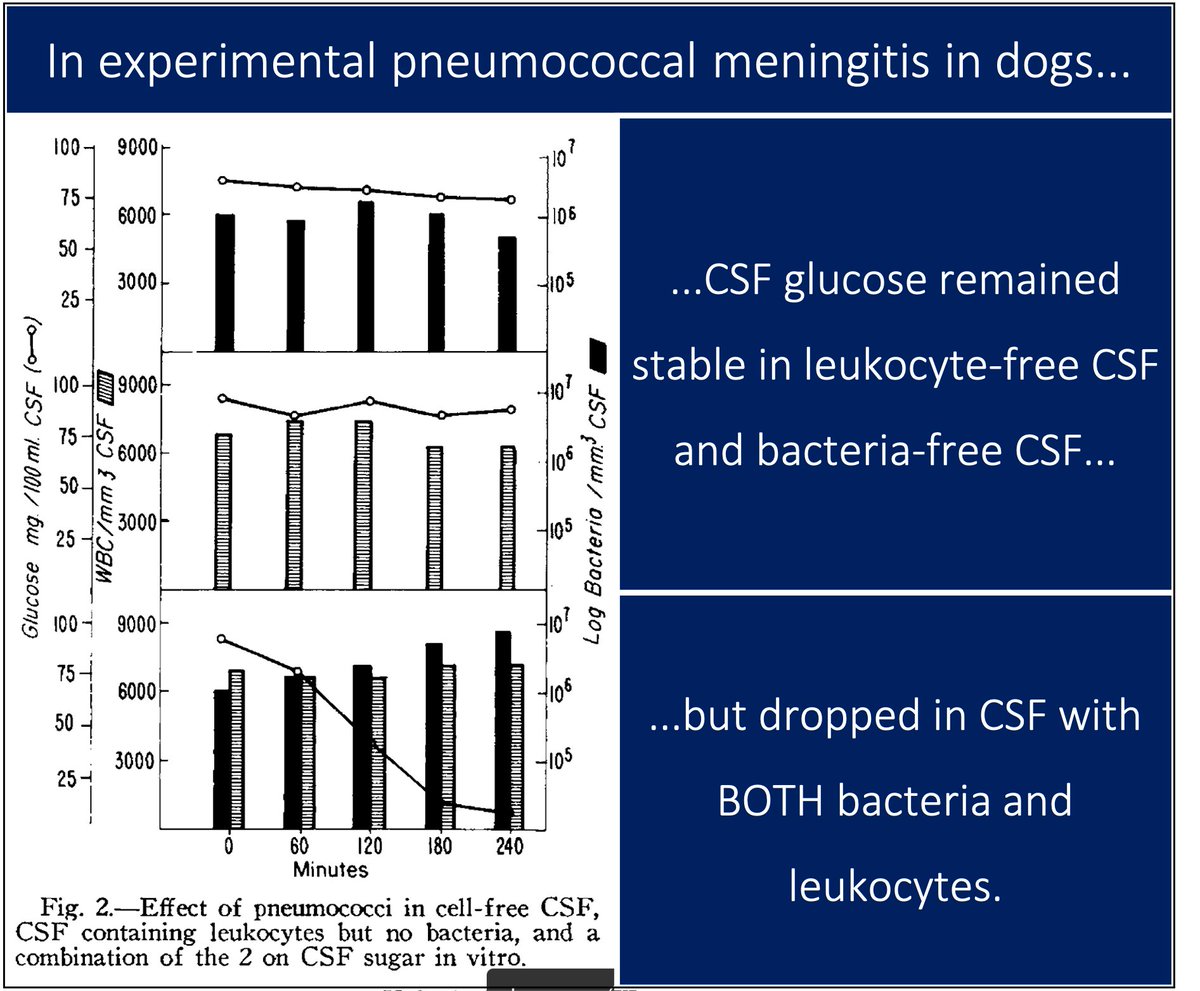
But bacterial consumption likely isn't sufficient.
For example, in 1961 Petersdorf and Harter reported that the fall in CSF glucose was attenuated in leukopenic dogs, even as the bacterial burden increased.
☞ WBCs appear necessary.
pubmed.ncbi.nlm.nih.gov/13734793/
But bacterial consumption likely isn't sufficient.
For example, in 1961 Petersdorf and Harter reported that the fall in CSF glucose was attenuated in leukopenic dogs, even as the bacterial burden increased.
☞ WBCs appear necessary.
pubmed.ncbi.nlm.nih.gov/13734793/
6/
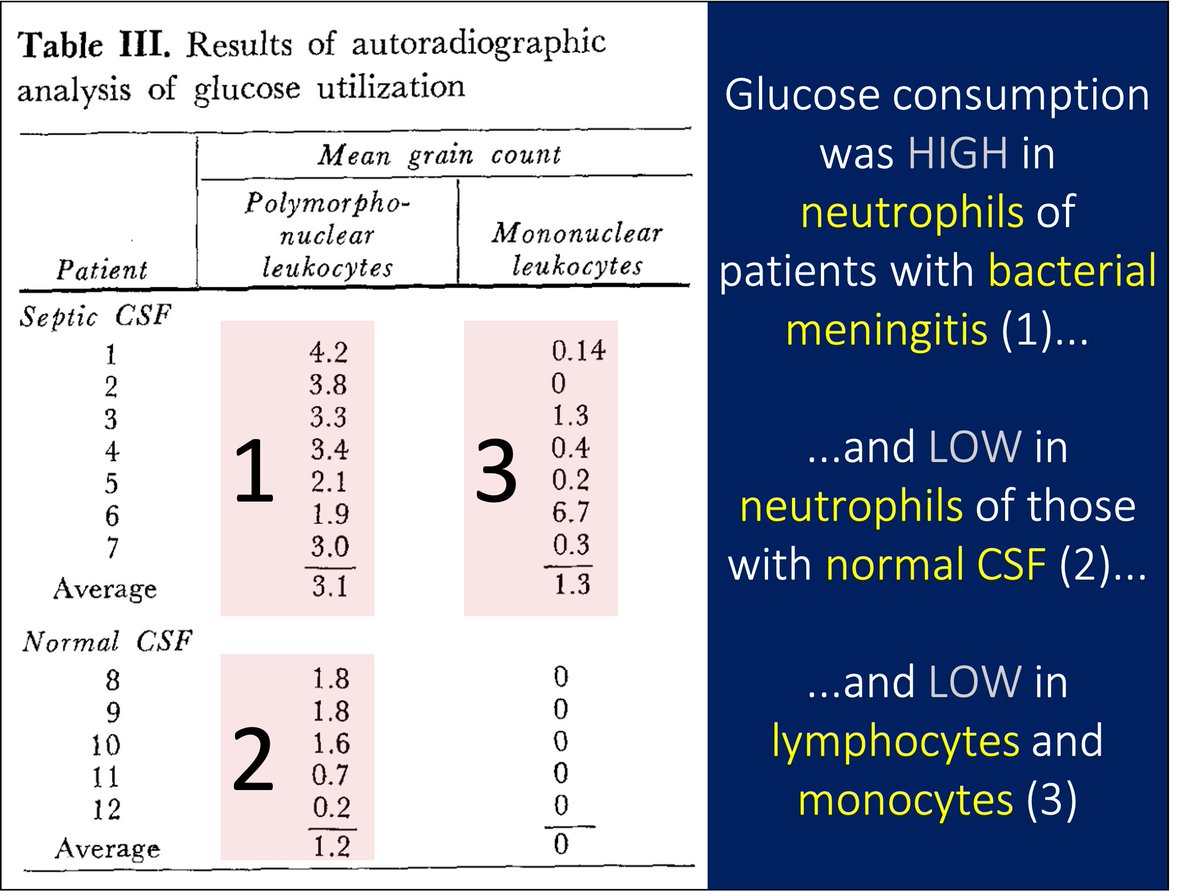
In fact, some studies suggest WBCs are an independent cause of hypoglycorrhachia, again via consumption.
But, the study in tweet 5 suggests a synergistic effect of bacteria and WBCs.
☞ Maybe you need bacteria AND neutrophils to drop CSF glucose.
pubmed.ncbi.nlm.nih.gov/6022180/
In fact, some studies suggest WBCs are an independent cause of hypoglycorrhachia, again via consumption.
But, the study in tweet 5 suggests a synergistic effect of bacteria and WBCs.
☞ Maybe you need bacteria AND neutrophils to drop CSF glucose.
pubmed.ncbi.nlm.nih.gov/6022180/
7/
But the "neutrophil/bacteria consume glucose" explanations also have problems.
Look again at the most causes of hypoglycorrhachia; most do not involve the combination of bacteria and neutrophils.
Something else must be going on.
This is where other hypotheses come in.
But the "neutrophil/bacteria consume glucose" explanations also have problems.
Look again at the most causes of hypoglycorrhachia; most do not involve the combination of bacteria and neutrophils.
Something else must be going on.
This is where other hypotheses come in.
8/
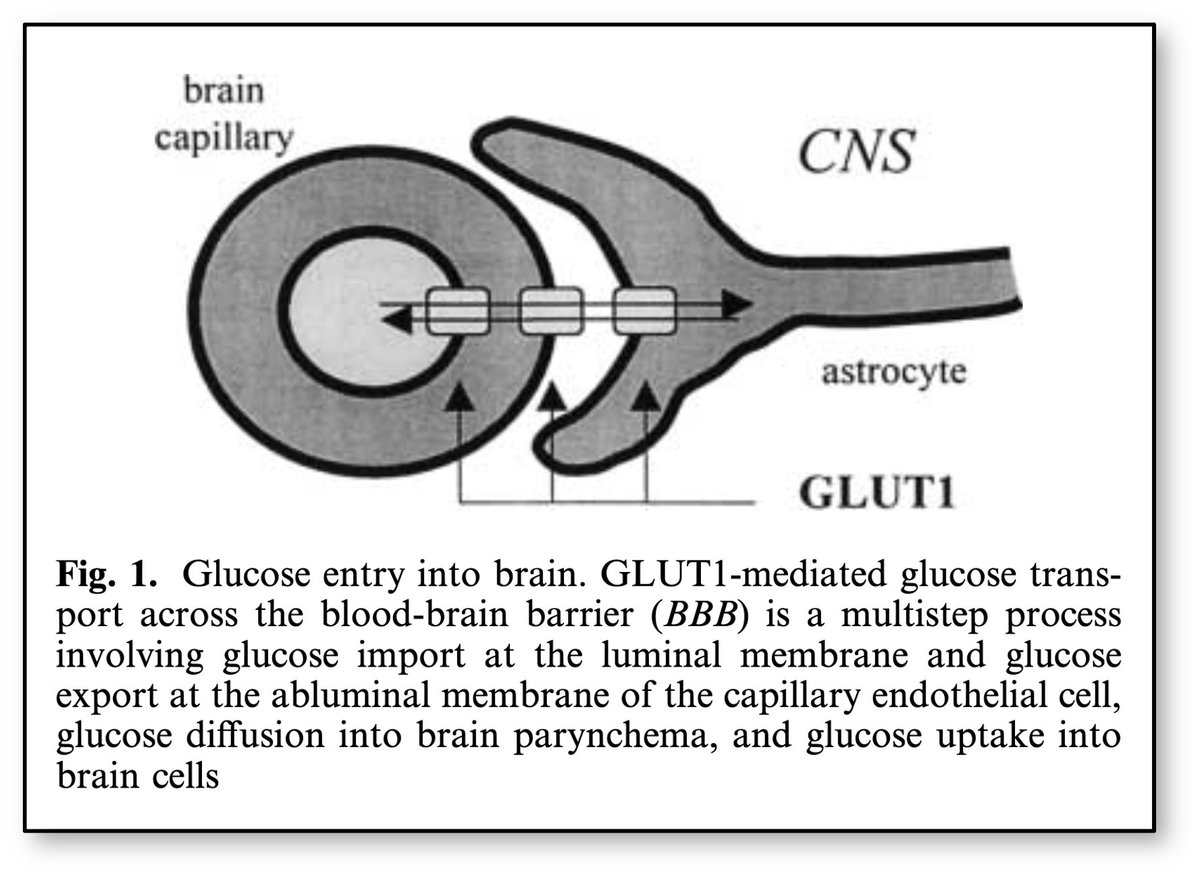
To understand the next explanation, we'll need to review glucose entry into the CSF.
Glucose crosses the blood-brain barrier into the CSF via the choroid plexus.
☞ Importantly, it uses facilitated diffusion via glucose transporter 1 (GLUT-1).
pubmed.ncbi.nlm.nih.gov/12029447/
To understand the next explanation, we'll need to review glucose entry into the CSF.
Glucose crosses the blood-brain barrier into the CSF via the choroid plexus.
☞ Importantly, it uses facilitated diffusion via glucose transporter 1 (GLUT-1).
pubmed.ncbi.nlm.nih.gov/12029447/
9/
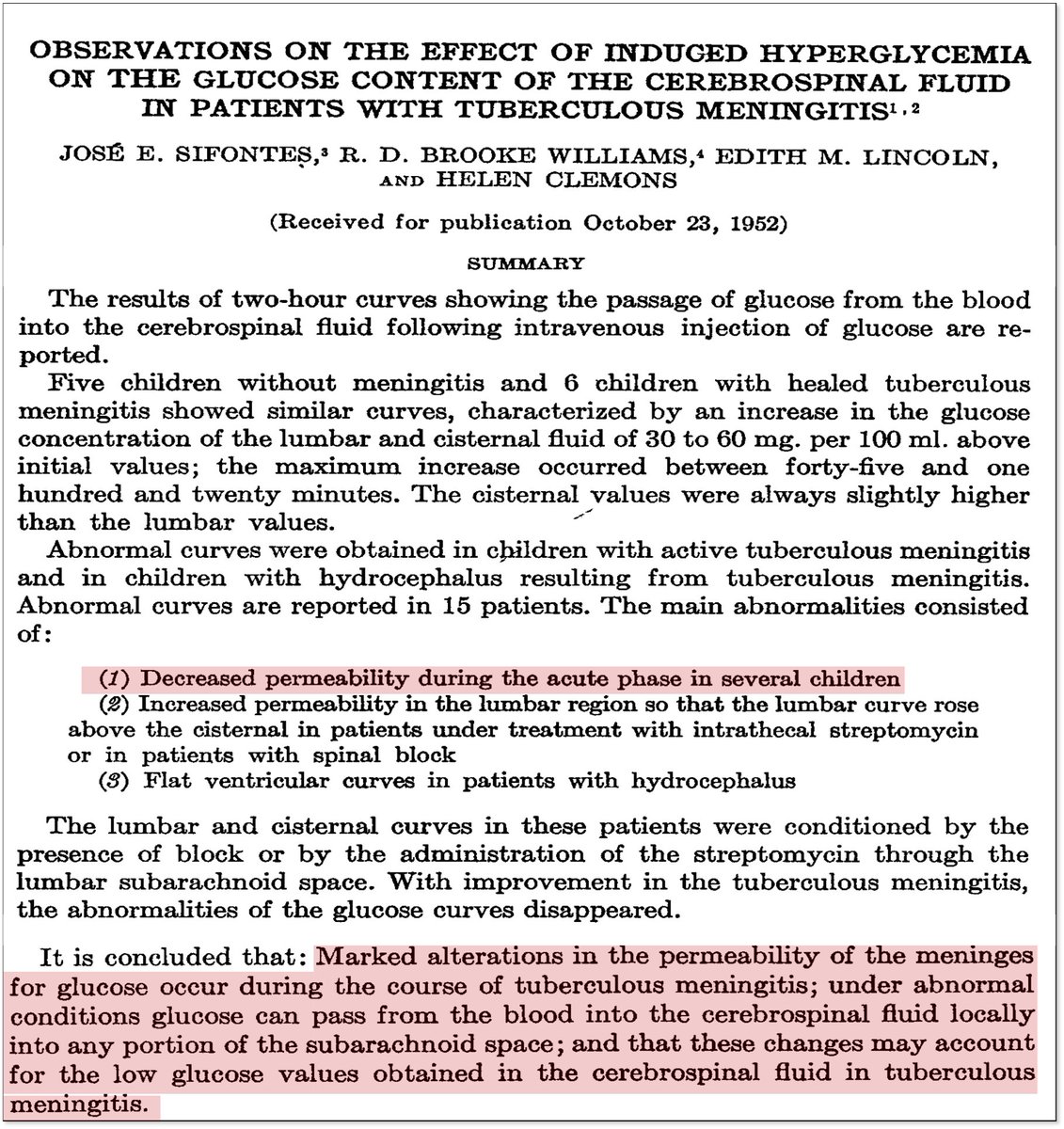
As far back as 1938, evidence has shown that disruption of the blood-brain barrier plays a role in hypoglycorrhachia, particularly in tuberculous meningitis.
In the subsequent decades, other studies have suggested the same.
linkinghub.elsevier.com/retrieve/pii/S…
pubmed.ncbi.nlm.nih.gov/13050945/
As far back as 1938, evidence has shown that disruption of the blood-brain barrier plays a role in hypoglycorrhachia, particularly in tuberculous meningitis.
In the subsequent decades, other studies have suggested the same.
linkinghub.elsevier.com/retrieve/pii/S…
pubmed.ncbi.nlm.nih.gov/13050945/
10/
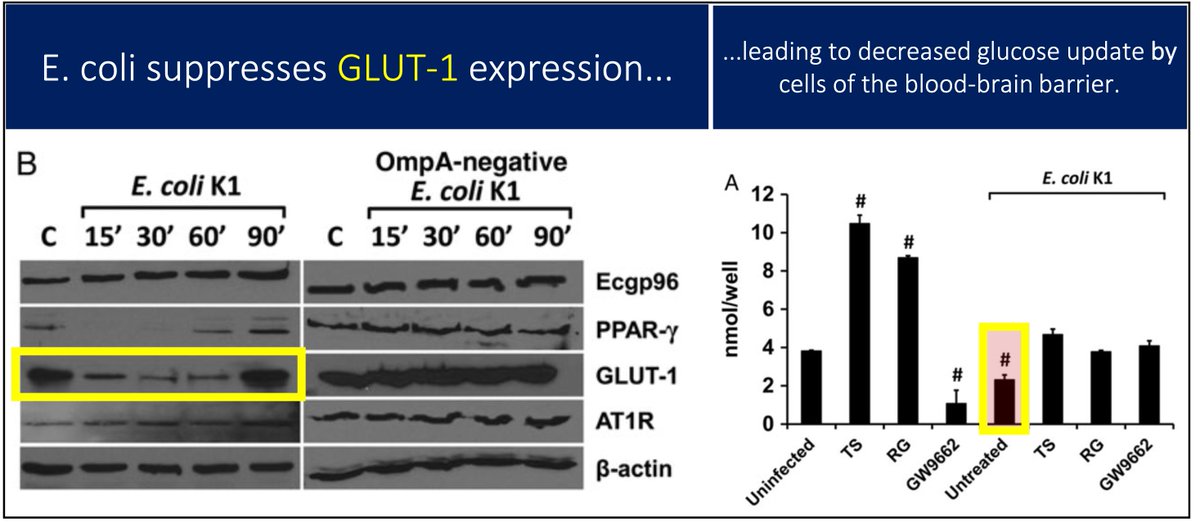
More recently it was shown that E. coli downregulates GLUT-1 in human blood-brain barrier cells, leading to inhibition of glucose uptake.
Whether similar downregulation occurs with other bacteria, I do not know.
pubmed.ncbi.nlm.nih.gov/27456707/
More recently it was shown that E. coli downregulates GLUT-1 in human blood-brain barrier cells, leading to inhibition of glucose uptake.
Whether similar downregulation occurs with other bacteria, I do not know.
pubmed.ncbi.nlm.nih.gov/27456707/
11/
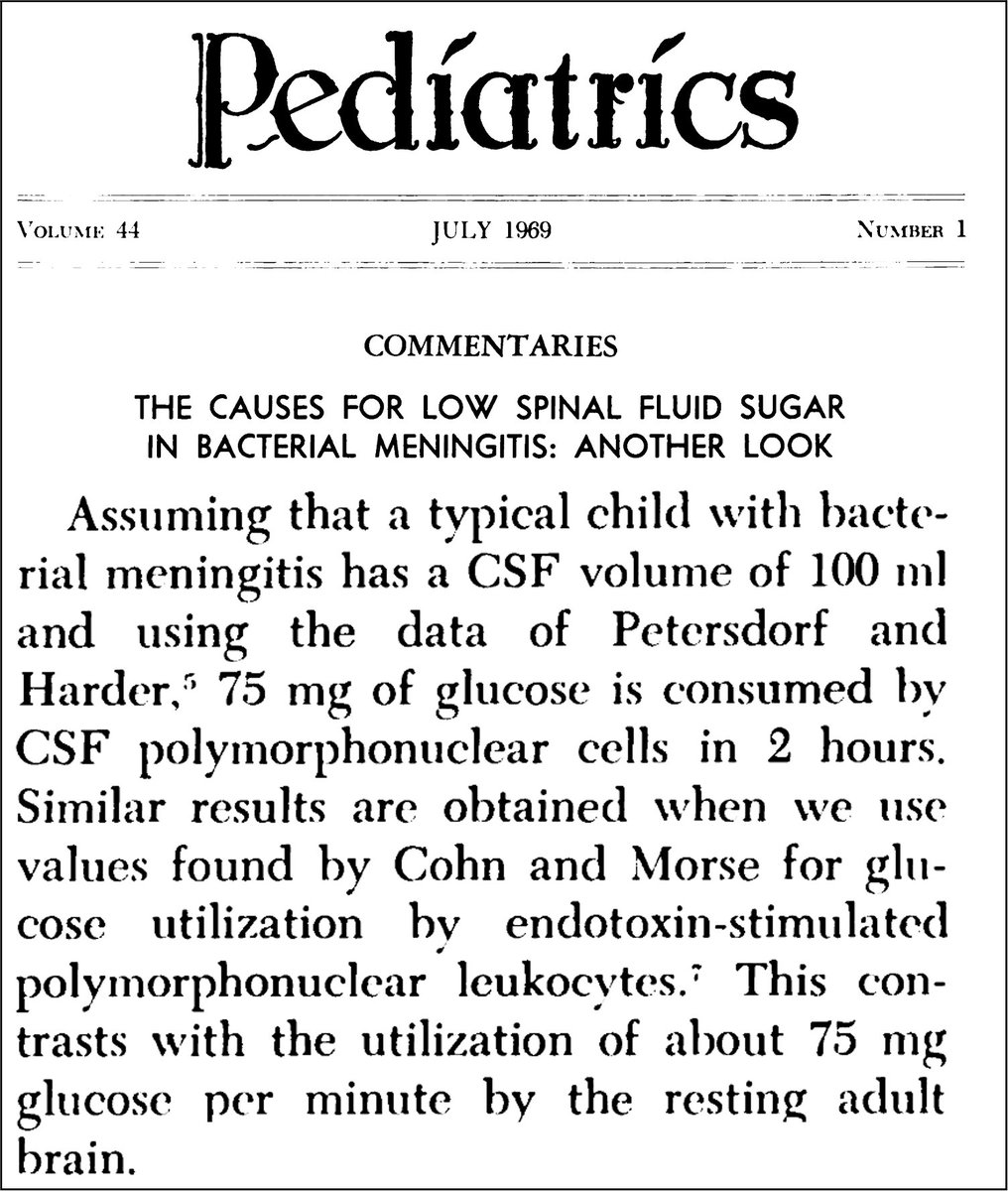
A final hypothesis suggests that our brains are consuming the glucose.
This was proposed in 1969 in a fantastic review by John Menkes. He argues that glucose consumption by bacteria/WBCs is just a fraction of brain cell consumption.
pubmed.ncbi.nlm.nih.gov/5795399/
A final hypothesis suggests that our brains are consuming the glucose.
This was proposed in 1969 in a fantastic review by John Menkes. He argues that glucose consumption by bacteria/WBCs is just a fraction of brain cell consumption.
pubmed.ncbi.nlm.nih.gov/5795399/
12/
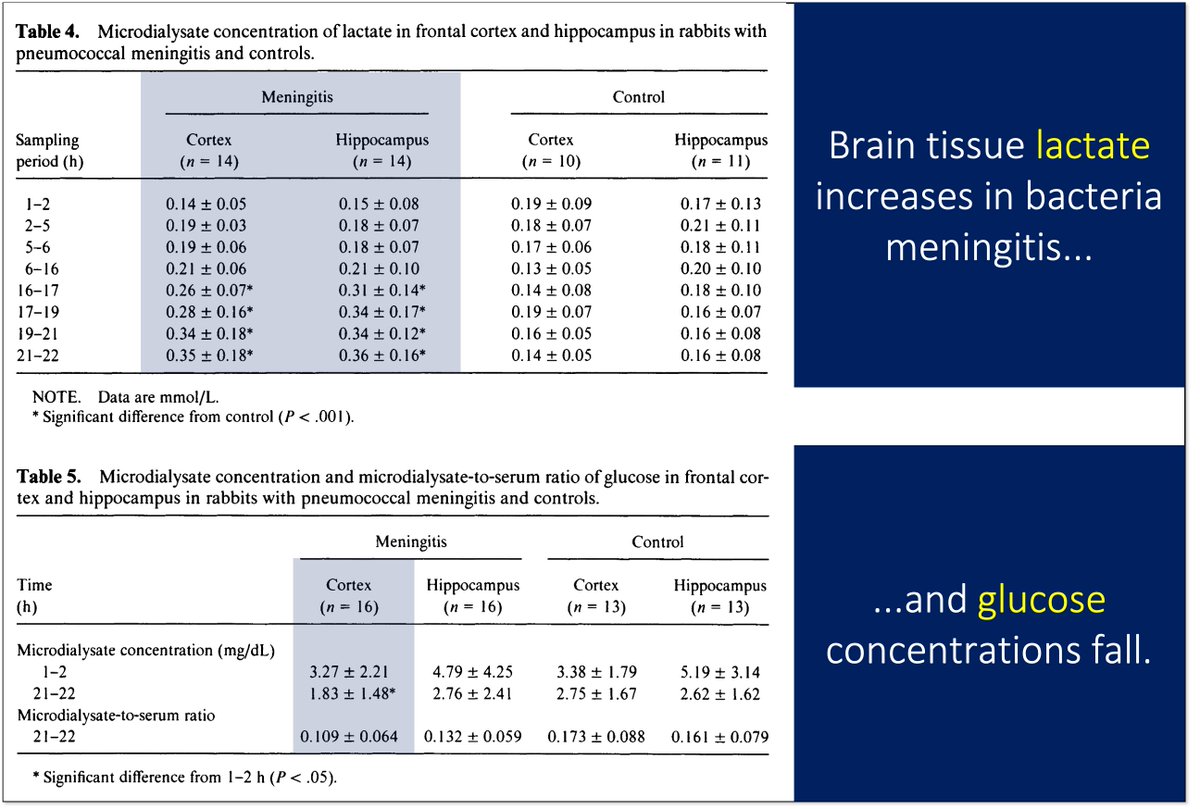
It's worth noting that these "something consumes glucose" explanations help explain the elevation in lactate seen in some forms of meningitis.
Some data support the brain (and not leukocytes/brain) as the source of lactate.
ncbi.nlm.nih.gov/pubmed/1500738
It's worth noting that these "something consumes glucose" explanations help explain the elevation in lactate seen in some forms of meningitis.
Some data support the brain (and not leukocytes/brain) as the source of lactate.
ncbi.nlm.nih.gov/pubmed/1500738
13/
In the end, the search for answers to "what causes hypoglycorrhachia?" is unlikely to provide a singular explanation. There are multiple mechanisms and/or each cause has a unique set of mechanisms.
Parsimony isn't always possible.
And that's ok.
In the end, the search for answers to "what causes hypoglycorrhachia?" is unlikely to provide a singular explanation. There are multiple mechanisms and/or each cause has a unique set of mechanisms.
Parsimony isn't always possible.
And that's ok.
14/14
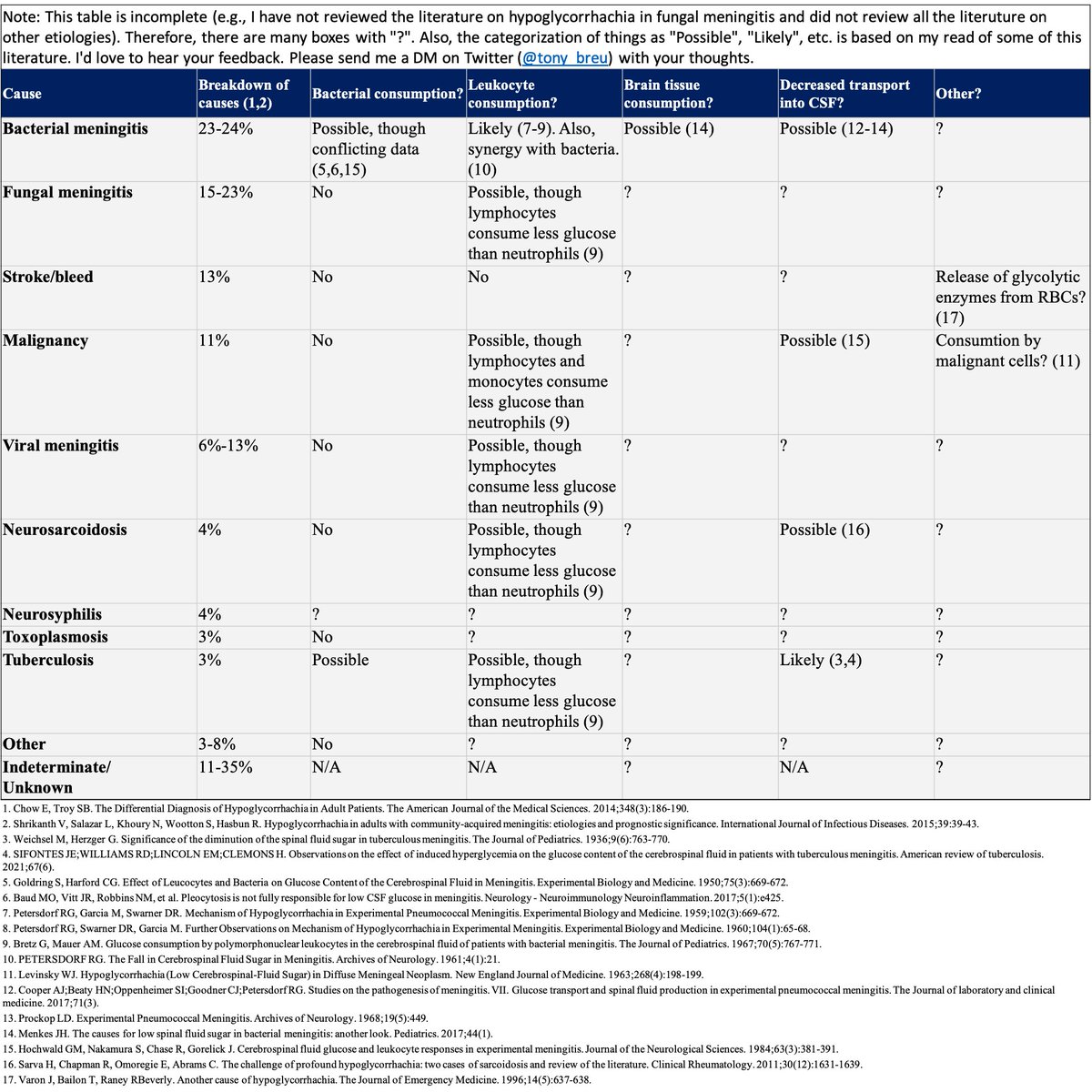
I'll close by sharing a table outlining the many routes to low CSF glucose, including...
🔹Bacteria and leukocytes and brain cells consumption of glucose...
🔹Blood-brain barrier damage limiting glucose entry...
...and others.
Better version: bit.ly/3a8nDk1
I'll close by sharing a table outlining the many routes to low CSF glucose, including...
🔹Bacteria and leukocytes and brain cells consumption of glucose...
🔹Blood-brain barrier damage limiting glucose entry...
...and others.
Better version: bit.ly/3a8nDk1
• • •
Missing some Tweet in this thread? You can try to
force a refresh