For this piece, I tried to gather together some thoughts about the serosurvey data coming out of India. There is a great deal of this data, and the messages are important but not always clear. Longish #thread. 1/n
scroll.in/article/986097…
scroll.in/article/986097…
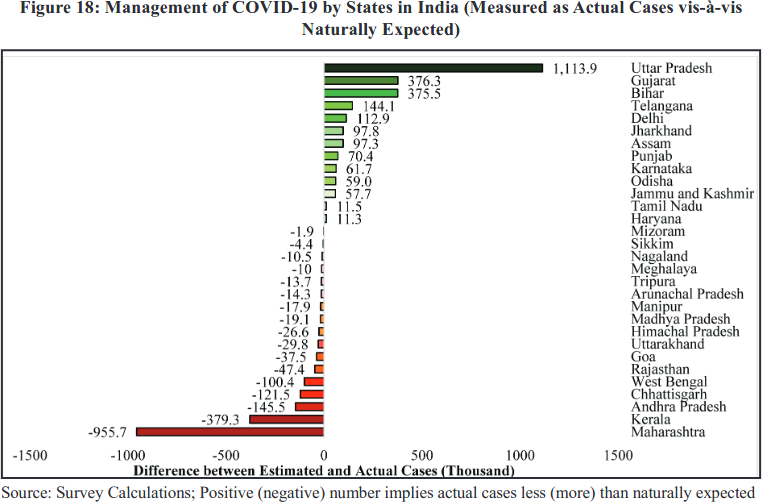
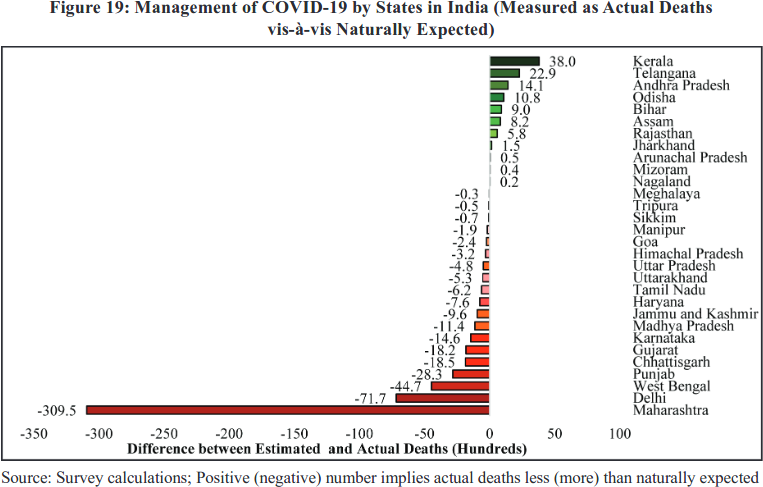
First, to see the bogus narratives you can construct when you ignore serosurvey data, you just have to look at Chapter 1 of the recent "Economic Survey". (This thread took just one example, but there are many.)
https://twitter.com/muradbanaji/status/1356280614442319882
Key message from the serosurveys? Extremely variable surveillance of infections *and probably deaths*. In some places, a decent proportion of infections are picked up; in others a tiny fraction. Some areas have seen a huge number of infections, but almost no recorded deaths.
If a region sees high spread (according to a serosurvey), but reports almost no fatalities, is it more likely that:
- people were magically spared?
- fatalities were not recorded?
science.thewire.in/health/bihar-c…
- people were magically spared?
- fatalities were not recorded?
science.thewire.in/health/bihar-c…
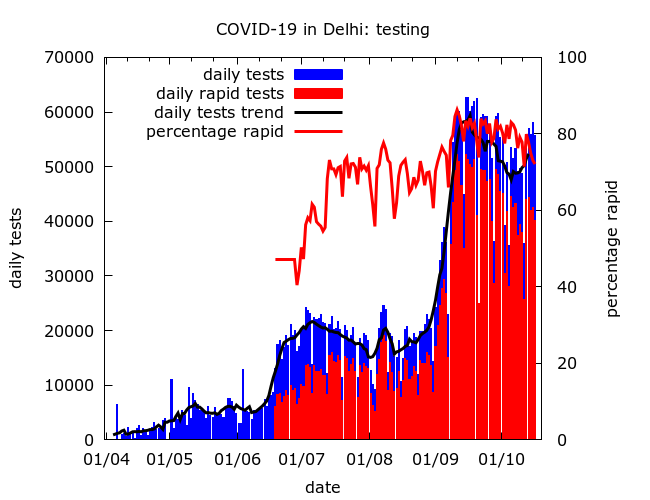
Testing is also now something of a game. The number of tests does not necessarily tell us how good detection is. The tests may be mistimed (e.g., test mainly after the wave has passed), or focussed on groups at low risk of infection.
We should be wary of interpreting falling test positivity as improving detection. Although this may *in general* be true, it is not necessarily the case. I tried to explain why in my recent piece for The Wire.
science.thewire.in/health/third-n…
science.thewire.in/health/third-n…
It may seem counterintuitive, but it's quite possible for the following all to occur:
- detection goes up in urban areas
- detection goes up in rural areas
- detection falls nationwide.
(I'll leave this one as a puzzle!)
- detection goes up in urban areas
- detection goes up in rural areas
- detection falls nationwide.
(I'll leave this one as a puzzle!)
When interpreting serosurvey data we should consider that old infections may be missed. E.g. analysis of Delhi's first 4 surveys here. (The recent survey 5 used a more sensitive test and effectively confirmed that earlier surveys were missing infections.)
https://twitter.com/muradbanaji/status/1327868673604763648
The serosurveys show consistently that housing poverty is strongly connected with rapid spread in urban areas. But the data doesn't tell us why. Poverty, discrimination and marginalisation can accelerate spread in many different ways and we need to disentagle these.
More generally, analysis of COVID data in India has shied away from tackling how COVID has interacted with inequality and marginalisation. The serosurveys only give us hints about this. (Chatted with @Rukmini about this here).
https://twitter.com/Rukmini/status/1337624633768509447
When interpreting the results of the surveys it's also important to keep an eye on details. How was sampling done? What could the biases be? Were these corrected for in the headline figures? This information is often missing...
...because of poor transparency. There's usually little technical detail until months later (if ever). Sometimes no info about how a population was sampled, or which test was used. Instead govt/private bodies drip feed the media bits of information heavily laced with propaganda.
There can be explicit political interference, as in the case of missing containment zone data from the first national serosurvey. Many of us still want to see this data. It is key to the story of the early epidemic.
economictimes.indiatimes.com/industry/healt…
economictimes.indiatimes.com/industry/healt…
Mainstream media is too often content to parrot official claims without verification. It may also add some misinformation of it's own. E.g. the absurd claim that the first national serosurvey showed 69% of rural Indians had been infected with COVID!
zeenews.india.com/india/69-4-peo…
zeenews.india.com/india/69-4-peo…
Main suggestions for those reporting on the surveys?
Ask:
- how was the population sampled?
- what test was used?
- were corrections done for sampling/test properties?
- breakdown by geography, housing, occupation, etc?
- implications for case detection/fatality rates?
Ask:
- how was the population sampled?
- what test was used?
- were corrections done for sampling/test properties?
- breakdown by geography, housing, occupation, etc?
- implications for case detection/fatality rates?
Final thoughts: the potential value of serosurvey data would be improved if more information was gathered (e.g., occupation, income, travel, access to info) + key technical info was shared rapidly. No need for a preprint right away - a technical report + raw data will do. n/n
• • •
Missing some Tweet in this thread? You can try to
force a refresh