
Our gamma delta + malaria paper got a "News and Views" @NatImmunol from the Harty's lab (probably a reviewer, hahaha). It was incredibly precise with the words, I'm deeply honored and I'm ready for a LONG🧵 on the paper! Let's go 1/
https://twitter.com/HartyLab/status/1358792709327097859
This story ain't new. As soon as the TCR was cloned, G9D2 T cells showed up in malaria context, not only that: they blast. A phenomena common when FSC and SSC were incredibly informative of activated phenotype and not all antibodies were available for FACS 2/ 

What that looked like in my hands was like this. Delta 2 TCR-PE purified human T cells (from PBMC) incubated with IL-2/IL-15 and P. falciparum 3d7 for 1d, 2d and 4 days. They not only blast, they become "grabby" with all RBCs in the absence of antibodies 3/
Well, my intention in 2015 wasn't to re-show GD kill Pf infected RBC culture, was to do a better mechanistic job looking how unconventional T cells use GNLY. As RBCs don't have MHC, nor modulate stress markers, they won't be targeted by NKs or CD8s easily 4/

Literature was at that stage in the figure below. But I thought there were experimental misconceptions and wanted to confirm that before moving on to protein assays 5/

So in our paper we shown that G9D2 upregulate expression of activation markers and GNLY in MFI and % in the presence of Pf in vitro (healthy donors) and in vivo. What impresses me is that PFN is not relevant to kill iRBC, and doesn't go up a lot either 6/
Surprisingly, with low IL-2/IL-15 incubation, even the G9D2 blast, they didn't kill iRBC in the first cycle, only after reinvasion two cycles (starting at 0.8%). @sabrina_absalon insisted to do smears after two cycles, after we thought of shutting down the project. 7/

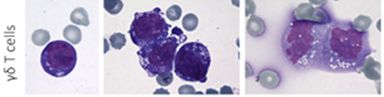
What we saw was quite interesting and defined the future of the story. It was really hard to find iRBC interacting with those G9D2 as the parasitemia was virtually 0, but you can grasp some ideas from this picture. Like, they're "seeing something" 8/

And whatever they are seeing, isn't restricted to iRBC. Most likely HMbPP, and RBCs "present it somehow". Well, more than one paper looked for BTN3A1 in RBC and didn't find it. I didn't bother to test, but Judy insisted. And I'm glad I was wrong. WB showing it there 9/

So, when I fixed-permeabilized the RBCs with PFA, the BTN3A (BT3.1) signal increased a lot (pRBC), suggesting a strong conformational dependency for the BT3.1 binding and explaining previous literature failure. iRBC loses membrane tension and becomes permeable, leaking PPs 10/

Importantly, blockage of GD TCR or BTN3A1 disrupted RBC lysis and degranulation, as well as the use o fosmidomycin to block the HMbPP pathway in iRBCs. Suggesting the participation of those three factors in the mechanism of killing 11/

We've shown before that Plasmodium consumption of cholesterol makes the iRBC susceptible to direct GNLY binding. So we used purified cytotoxic proteins and shown GNLY can disrupt parasite growth and is aided by GzmB and PFN 12/ nature.com/articles/s4159…
I still couldn't explain why it took 2 cycles for the G9D2 to kill the iRBCs. I reached out to @eberlmat and he taught me all sorts of ways to activate and keep G9D2 cytotoxic ex vivo, and I came up with 200IU IL-2/25ng/mL IL-15 for 4-5 days as best 13/

Many papers in cancer studying G9D2 uses CD107a degranulation instead of actual cytotoxicity in their papers, and I imagine that they could benefit from that stimulation protocol and LDH or IFA. It took me long optimization to see they kill ex vivo 14/ @forum_gd
Here's how the parasites look after the killing. You can add the activated G9D2 even 1h and add PFA, do IFAs, ImageStream, look at doublets by flow. It is amazing how they work. Note that in the presence of HMbPP (iRBCs) they become fratricidal. So they kill each other too. 15/

@prasannaj77 lab (collaborator-2017) has shown that to have those cells activated for long might be detrimental. They probably help in the beginning, and their pre-circulating levels are a strong correlate of sterile protection in Seder's vaccine tests. 16/
The increase in frequency of CD16 receptor G9D2 cells is good for patients. So, using the "grabby" gamma deltas from my smears and other data, Carol Junqueira took my project after I was let go, refined the methods and the data by a lot and found the phagocytosis 17/
In Patrick Brennan's lab, I participated in an innate T cells transcriptome project and I do not recall the machinery for phagocytosis coming up in healthy D2 T cells, but we weren't focused on that, nor sorted CD16+D2+ cells. 18/ nature.com/articles/s4146…
Junqueira shown that the blockage of CD16, CD36 and GD TCR impacts the antibody dependent phagocytosis, and the internalization not only increased in the presence of Pf patient sera, but the phagocyted cells have the dye reduced in time, suggesting lysosomal degradation. 19/

Elegantly, Carol demonstrated that the mechanisms for cytotoxicity and phagocytosis seem to be independent. When you block degranulation you still get phagocytosis, and vice versa. Interestingly, ADCC didn't seem to play a role in G9D2. But as NK cells have CD16, 20/

do they also phagocyte given the circumstances? In literature and our hands, NK cells reacted a lot to iRBCs. They have a similar transcription program to G9D2s on the cytotoxic end, respond to IL-2/IL-15 similarly too. We hope this knowledge can lead to a lot of studies! 21/
It is noteworthy that from my first data showing up mid 2016 until now, Michael Walch group (previous Judy's postdoc) and @FeeneyLabUCSF complemented our findings in amazing papers that you should definitely look up. 22/22
jimmunol.org/content/204/7/…
pubmed.ncbi.nlm.nih.gov/33085728/
jimmunol.org/content/204/7/…
pubmed.ncbi.nlm.nih.gov/33085728/
@threadreaderapp unroll
I forgot to add the paper link in the thread at all, here it is, and I'd rather use Junqueira and Polidoro et al, but do as you may hahaha. Cheers, and thank you if you read this until here.
nature.com/articles/s4159…
nature.com/articles/s4159…
• • •
Missing some Tweet in this thread? You can try to
force a refresh


