Thoughts on vaccine effects:
When evaluating the effects of vaccines there are two complementary forms of evaluation:
1. Measuring the direct effects of the vaccine on the individuals vaccinated
2. Measuring the overall impact of the vaccine program on an entire population
>>
When evaluating the effects of vaccines there are two complementary forms of evaluation:
1. Measuring the direct effects of the vaccine on the individuals vaccinated
2. Measuring the overall impact of the vaccine program on an entire population
>>
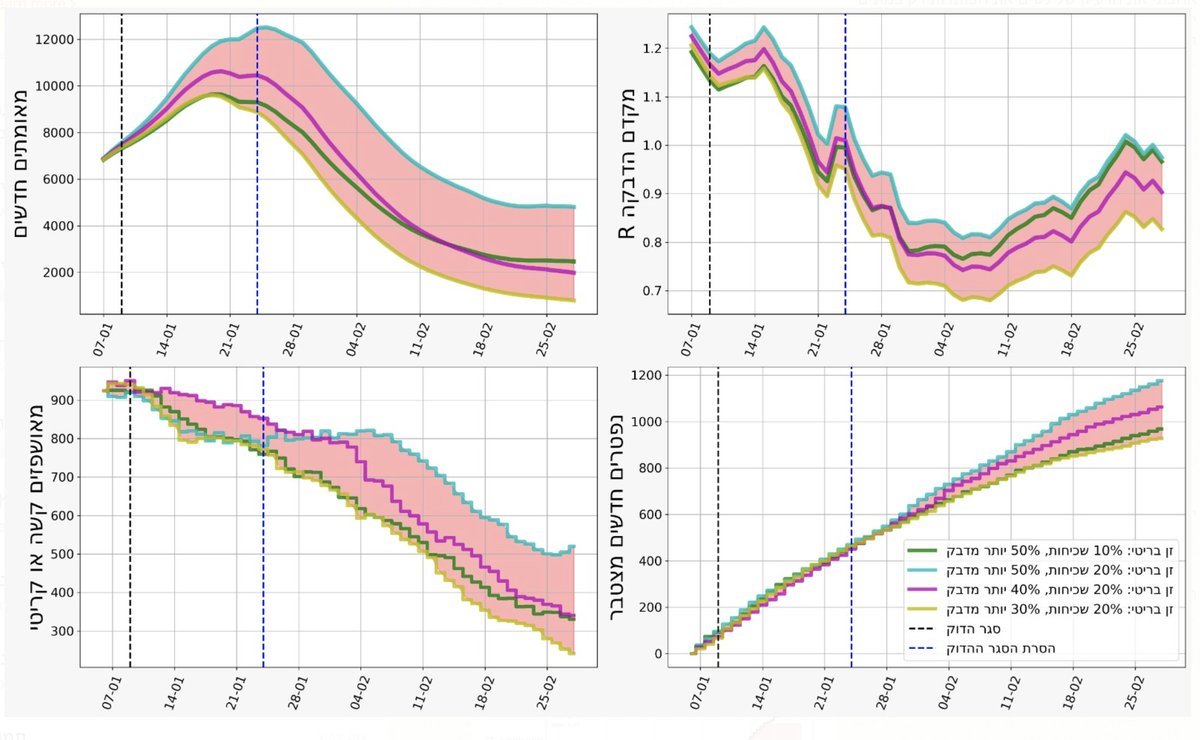
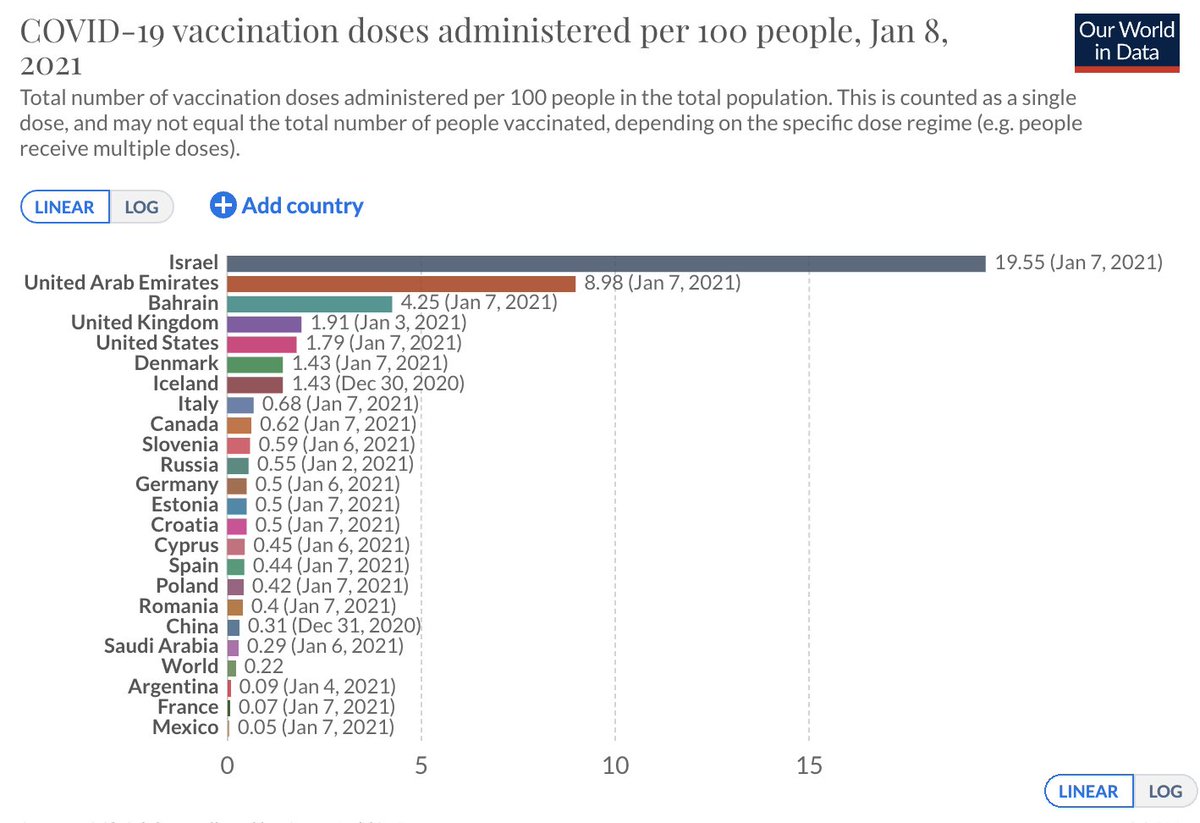
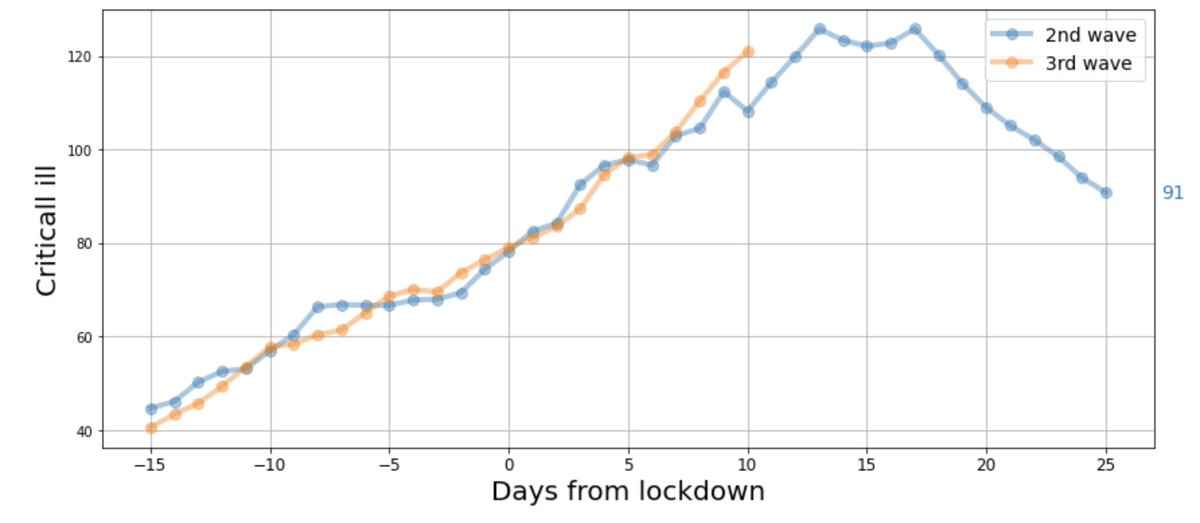
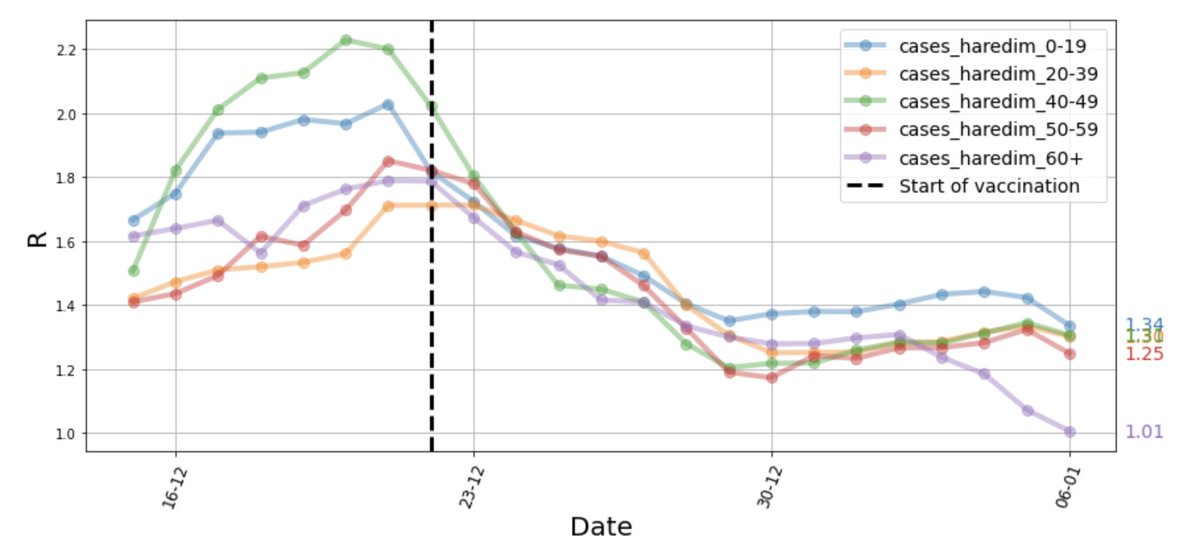
We focused on #2, aiming to show the real-life impact of a vaccination campaign on the dynamics of the COVID-19 pandemic at the entire population / country level
Preprint here: tinyurl.com/jyjho4v9
>>>
Preprint here: tinyurl.com/jyjho4v9
>>>

For example, we showed the impact of a vaccine program when a large proportion of the elderly population of a city is vaccinated, where the impact is measured in terms of total number of cases and hospitalizations among that city’s population
>>>
>>>
This differs from the imporatnt study of @RanBalicer @mlipsitch @_MiguelHernan & colleagues @NEJM showing the level of protection an elderly person can expect once vaccinated: nejm.org/doi/full/10.10…
>>>
>>>
The impact of a vaccine program depends not only on vaccine effectiveness, but also on other factors, including national vaccine coverage, vaccine allocation in subgroups of different risk levels, and social mixing of groups that may affect transmission by indirect effects
• • •
Missing some Tweet in this thread? You can try to
force a refresh