
VACCINE ESCAPE OF VARIANTS vs Pfizer-BioNTech & NIH-Moderna: Troubling new peer-reviewed paper shows even 2-dose recipients have serious trouble neutralizing the #B1351 🇿🇦 variant—as little as vs old SARS & bat coronavirus. #P1 is poor too. 1-dose worse. Lots of graphs🧵 #COVID19 

2) First let’s cover some good news, that having 2 doses clearly MUCH MUCH better than 1 dose alone of either the Pfizer or Moderna vaccines versus neutralizing the classic #SARSCoV2 common strain.
cell.com/cell/pdf/S0092…
cell.com/cell/pdf/S0092…
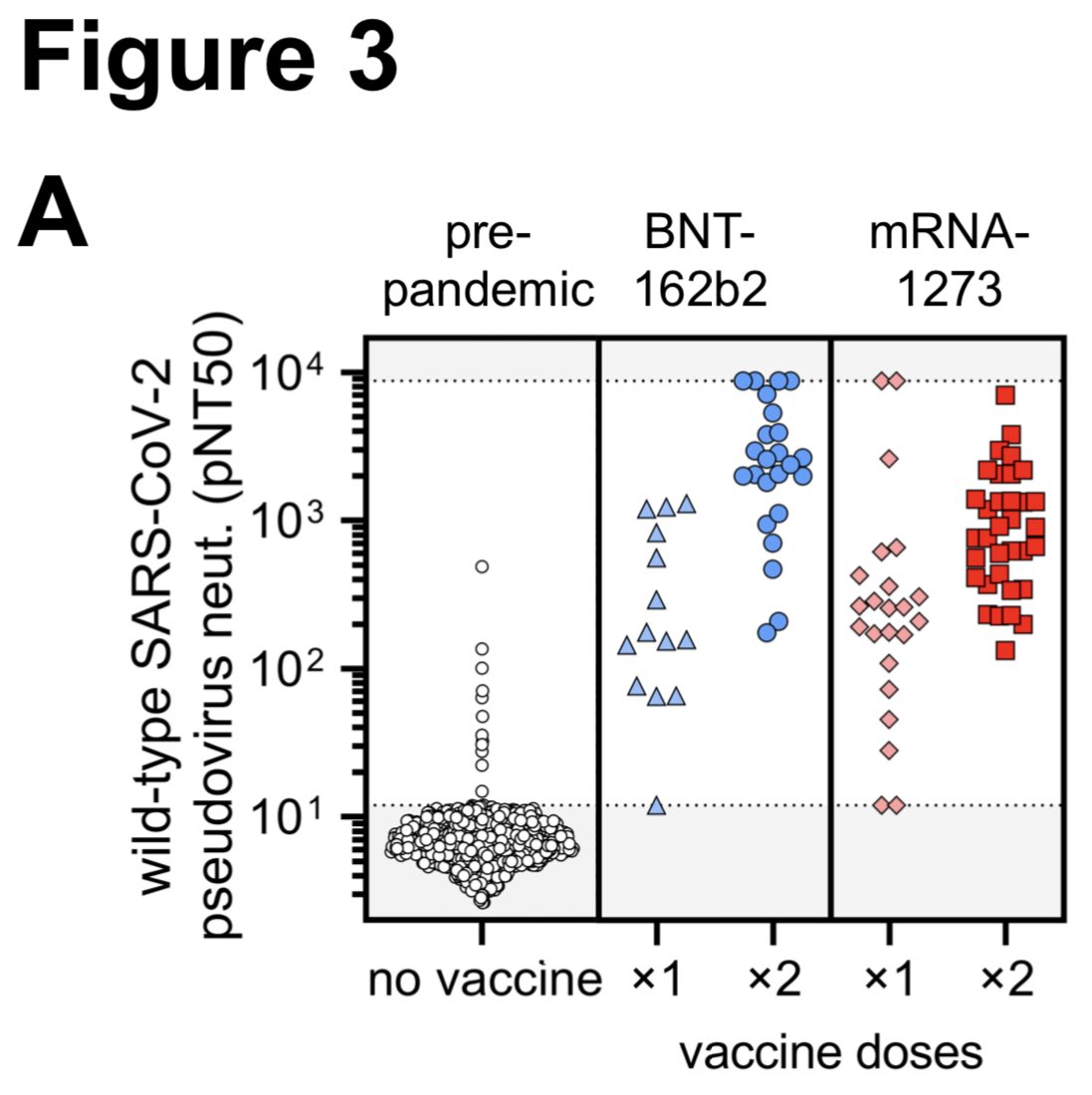
3) Notably, notice how much stronger in neutralization the blood of people with 2 doses of either Pfizer (dark blue) or Moderna (dark red) is versus the 1 dose of each. Note the logarithmic y-axis. So the difference is even greater.

5) The neutralization curves from 2-doses BNT162b2 vaccine of wild-type SARS-CoV-2 to variant pseudoviruses: poor overlap=bad.
#B117 is pretty good. California #B1429 pretty good. Brazil #P1 & #B1351 have more trouble.
But this is just one person—let’s looks at more people:
#B117 is pretty good. California #B1429 pretty good. Brazil #P1 & #B1351 have more trouble.
But this is just one person—let’s looks at more people:

6) Now let’s look at many folks with 1 and 2 doses of the Pfizer-BioNtech vaccine... 1 dose much lower than 2 doses. #B1351 and #P1 poor neutralization—akin to old 2003 SARS & other bat coronavirus that are only ~75% related to #SARSCoV2!
(%🧬wise—akin humans & elephants close)
(%🧬wise—akin humans & elephants close)

7) Now let’s look at many folks with 1 or 2 doses of the NIH-Moderna vaccine... 1 dose still much lower than 2 doses. And #P1 and #B1351 also agains problematic. But Moderna had slightly better performance vs Pfizer... let’s look at next graph...

8) let’s focus on just Pfizer and exactly how much relative fold decrease 2-dose vaccinated person had against each variant in neutralization vs the common #SARSCoV2. Values <3x is not major difference.
#P1 is moderately poor at 6.7x drop, but #B1351 has 34x to 42x drop! Wow.
#P1 is moderately poor at 6.7x drop, but #B1351 has 34x to 42x drop! Wow.

9) now let’s turn on just Moderna and how much fold decrease 2-dose vaccinated persons had against each variant in neutralization vs common #SARSCoV2.
#P1 is moderately poor at 4.5x drop (Pfizer had 6.7x drop), but #B1351 has 19-27x drop! (Better than Pfizer 34-42x). Still wow.
#P1 is moderately poor at 4.5x drop (Pfizer had 6.7x drop), but #B1351 has 19-27x drop! (Better than Pfizer 34-42x). Still wow.

10) To be clear, these fold drops in neutralization does not equal vaccine % efficacy drops directly. For example, #B117 has often had ~2x neutralization drop but usually similar % efficacy. T-cell immunity is also not included. But >6x we often see some efficacy changes.
11) Overall, it looks like:
📌really need 2 doses for maximal protection (time gap not evaluated here)
📌Vaccines looks generally good against #B117 & #B1429 (CA variant)
📌#P1 moderately poorer
📌#B1351 looks worrisome. #B1351 results looks akin to unrelated coronaviruses.
📌really need 2 doses for maximal protection (time gap not evaluated here)
📌Vaccines looks generally good against #B117 & #B1429 (CA variant)
📌#P1 moderately poorer
📌#B1351 looks worrisome. #B1351 results looks akin to unrelated coronaviruses.
12) “Five of the 10 pseudoviruses, harboring receptor-binding domain mutations, including K417N/T, E484K, and N501Y, were highly resistant to neutralization.
13) “Cross-neutralization of B.1.351 variants was comparable to SARS-CoV and bat-derived WIV1- CoV, suggesting that a relatively small number of mutations can mediate potent escape from vaccine responses.”
14) “these results highlight the potential for variants to escape from neutralizing humoral immunity and emphasize the need to develop broadly protective interventions against the evolving pandemic.”
15) Another preprint recently found similar worrisome results for #B1351 neutralization by Pfizer & Moderna vaccinated? Yes—preprint by Columbia/NIH group also found 10-12x fold drop—again huge.
A Harvard colleague whispered to me: it’s “very concerning”
biorxiv.org/content/10.110…
A Harvard colleague whispered to me: it’s “very concerning”
biorxiv.org/content/10.110…

16) This same study also found problems of certain monoclonal antibodies drugs against #B1351. But not all.

17) What about convalescent plasma therapy versus the #B1351 and #B117 variants? Decent for #B117. Again super poor for #B1351. This South Africa 🇿🇦 #B1351 variant is quite “concerning” my immunology colleague said (someone who doesn’t usually get worried a lot)

18) I want to emphasize — PLEASE PLEASE PLEASE still take the vaccine. The #B1351 variant and #P1 variant are still very very rare in the US and Europe (knock on wood). The vaccines work great for all the other major variants of #B117 and #B1429 (California). So pls #vaccinate
19) on the flip side, T cell mediated immunity via CD4+ & CD8+ T cell responses in convalescent #COVID19 subjects or mRNA vaccinees are not substantially affected by mutations found in the SARS-CoV-2 variants #B117 #P1 #Calc20 (aka #B1429g or #B1351.
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
20) to be clear, both T cells and antibody neutralization important for immune response to the coronavirus. Each pathway offers a degree of protective immunity, but not as good as if both pathways are at maximal. That’s why some immunologist colleagues still whispering concerns.
21) the good thing is that it seems for J&J vaccine, it is still good for #B1351 - still 81% against severe disease in South Africa 🇿🇦 trial component. See thread 🧵
https://twitter.com/DrEricDing/status/1366619383997607941
22) and the Novavax vaccine still worked for the #B1351 South Africa variant, albeit attenuated at 55% overall. Severe is near 100%. We don’t have #P1 in this Novavax trial.
https://twitter.com/DrEricDing/status/1370205587066253313
23) The most head-scratching thing is why did this earlier study by Pfizer of Prizer vaccine show it was pretty good for #B1351 & #P1 for antibody neutralization whenever the 2 new studies by Columbia/NIH & Harvard groups show it is not. My immunologist colleagues are perplexed.
https://twitter.com/DrEricDing/status/1369288725843283970
24) My colleague thinks maybe the study by Pfizer tested a different type of pseudovirus (unclear) or Pfizer maybe excluded low responders in their own study. We think the NIH-Columbia group and Harvard-South Africa (top post) studies are likely better with no industry conflict.
25) A lot of people still don’t understand mRNA vaccines like Pfizer and Moderna. So here is a more simple explainer.
https://twitter.com/DrEricDing/status/1370106365784506370
26) Reminder: please don’t relax too soon. This pandemic isn’t over. I can be over sooner if we work together and not dismiss safety measures until we are vaccinated sufficiently. Until then mask and ventilate. 🙏
https://twitter.com/DrEricDing/status/1370726658735505408
27) What happens if we ignore #COVID19 pandemic? Brazil 🇧🇷 crisis happens. This is the effect of the unchecked transmission of #P1 variant. Epic crisis.
https://twitter.com/DrEricDing/status/1372005826383204353
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















