Happening now at #RPA21:
The Challenges of Social Media Education: A data-driven specialty-specific introspection
rpa2021.onlineeventpro.freeman.com/live-stream/19…
I'm live on the RPA platform and Twitter for your questions
The Challenges of Social Media Education: A data-driven specialty-specific introspection
rpa2021.onlineeventpro.freeman.com/live-stream/19…
I'm live on the RPA platform and Twitter for your questions

1/#rpa21
My disclosures
I created Nephrology On-Demand in 2010
I launched @NODanalytics in 2015
I made @NODanalytics free for educational use in 2018
I created NephTwitterArchive.com to mitigate the perils of customized search
goo.gl/mfziXG
My disclosures
I created Nephrology On-Demand in 2010
I launched @NODanalytics in 2015
I made @NODanalytics free for educational use in 2018
I created NephTwitterArchive.com to mitigate the perils of customized search
goo.gl/mfziXG
2/#rpa21
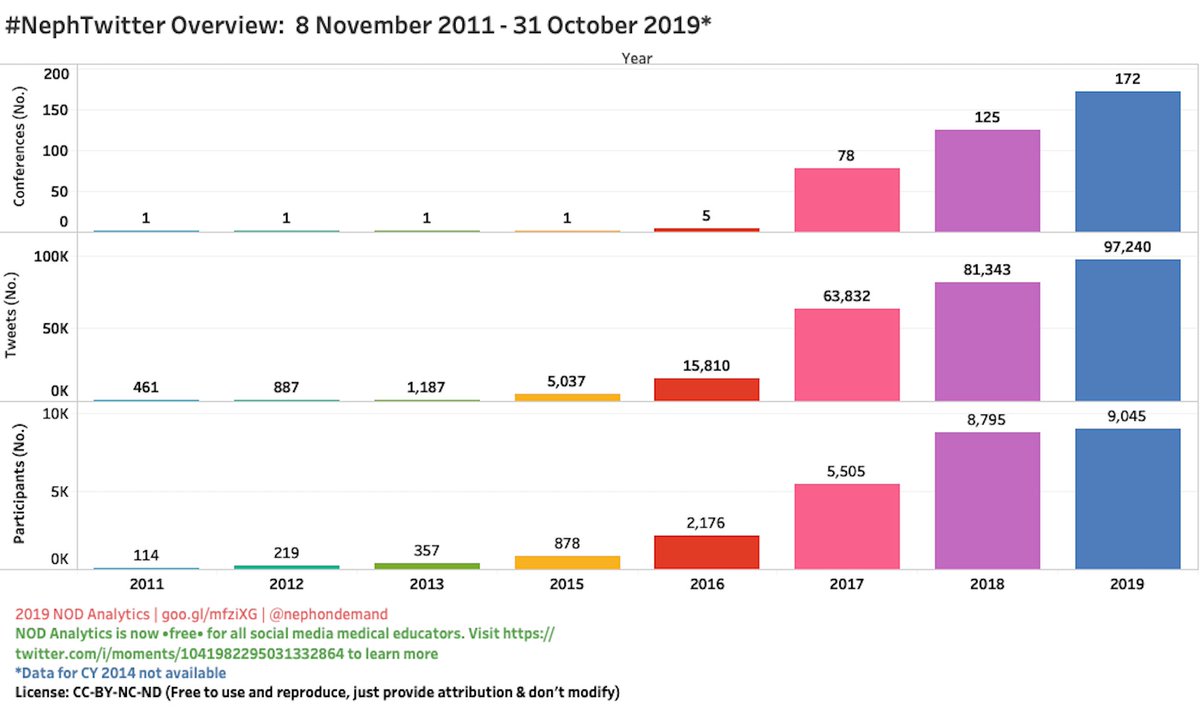
Many specialties are gravitating to Twitter for education & learning.
Some are more advanced than others; it is very evident that #NephTwitter is far more advanced than other specialties: longer experience w/#SoMe education & more offerings.
Many specialties are gravitating to Twitter for education & learning.
Some are more advanced than others; it is very evident that #NephTwitter is far more advanced than other specialties: longer experience w/#SoMe education & more offerings.
3/#rpa21
Those specialties that are beginning with Twitter-based education are in the "honeymoon period" -- you know, a period where everything looks fine and dandy.
More experienced specialties (#NephTwitter) are able to see the challenges and obstacles that can hinder learning
Those specialties that are beginning with Twitter-based education are in the "honeymoon period" -- you know, a period where everything looks fine and dandy.
More experienced specialties (#NephTwitter) are able to see the challenges and obstacles that can hinder learning

4/#rpa21
We face 3 challenges in Twitter-based learning:
• gender inequality
• polarization of groups
• perils from customized search
Turning a blind eye to these challenges will worsen our learning communities (that's not opinion anymore...it's already happening).
We face 3 challenges in Twitter-based learning:
• gender inequality
• polarization of groups
• perils from customized search
Turning a blind eye to these challenges will worsen our learning communities (that's not opinion anymore...it's already happening).

5/#rpa21
The easiest solution is to walk away from Twitter. All of us learned during our formative years w/o Twitter.
Walking away, however, would be going against the tidal wave that is fueling #NephTwitter. Each year, more nephrologists and conferences invest in Twitter.
The easiest solution is to walk away from Twitter. All of us learned during our formative years w/o Twitter.
Walking away, however, would be going against the tidal wave that is fueling #NephTwitter. Each year, more nephrologists and conferences invest in Twitter.


6/#rpa21
So our goal is to understand each of these challenges, measure their effect on the #nephTwitter learning communities, and devise solutions to bring us to a better place.
So our goal is to understand each of these challenges, measure their effect on the #nephTwitter learning communities, and devise solutions to bring us to a better place.

7/#rpa21
Challenge #1: Gender inequality
This should've never happened. All of #nephTwitter should have made a concerted effort to keep gender equality front-and-center when developing various Twitter learning communities. Alas, we didn't do that and now we have this scourge.
Challenge #1: Gender inequality
This should've never happened. All of #nephTwitter should have made a concerted effort to keep gender equality front-and-center when developing various Twitter learning communities. Alas, we didn't do that and now we have this scourge.

8/#rpa21
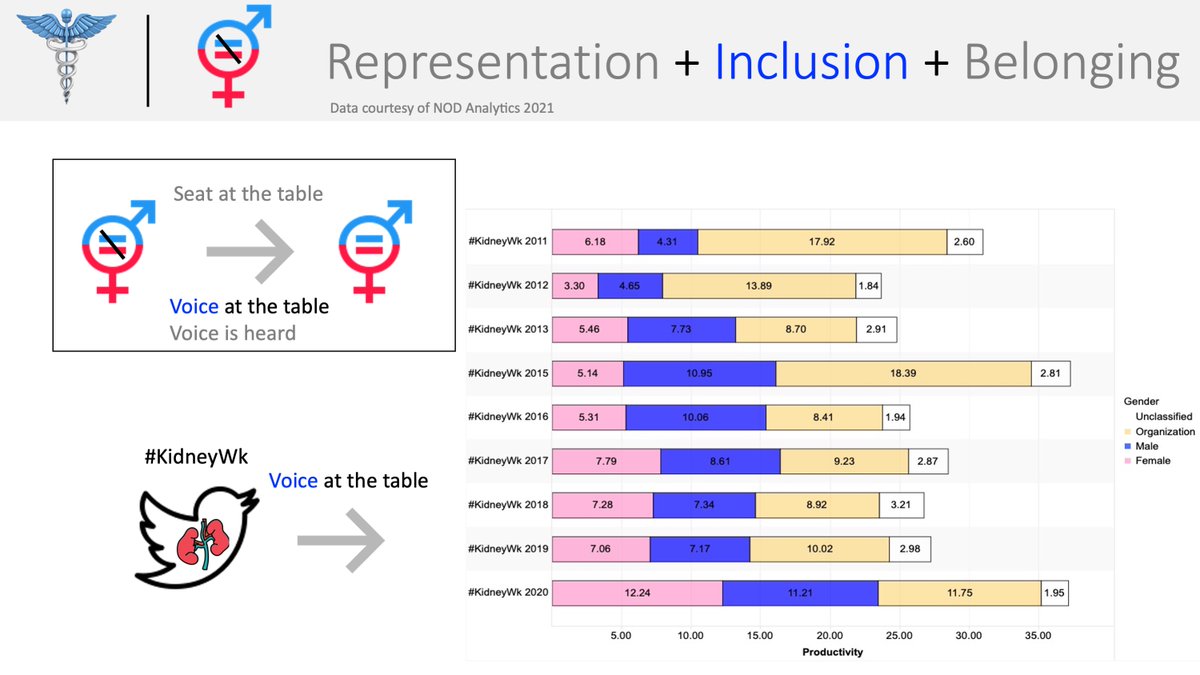
Achieving gender equality requires successes in 3 areas: representation, inclusion, and belonging.
@lizandmollie
We'll look at data from @ASNKidney and #KidneyWk to see how well (not) gender equality is being achieved.
Achieving gender equality requires successes in 3 areas: representation, inclusion, and belonging.
@lizandmollie
We'll look at data from @ASNKidney and #KidneyWk to see how well (not) gender equality is being achieved.

9/#rpa21
On the left: representation of female scientists in the @ASNKidney membership roll (#s & %): a growth rate of ~1% per year since 2015.
On the right: representation of female scientists in #KidneyWk (#s & %): +1% per year since 2015
Why is the latter such a big problem?
On the left: representation of female scientists in the @ASNKidney membership roll (#s & %): a growth rate of ~1% per year since 2015.
On the right: representation of female scientists in #KidneyWk (#s & %): +1% per year since 2015
Why is the latter such a big problem?


10/#rpa21
In the real world, there are challenges towards achieving equal gender representation: geographic, financial, language, and time. These aren't excuses, just realities that the good folks @ASNKidney are trying to overcome to achieve parity in the membership roll.
In the real world, there are challenges towards achieving equal gender representation: geographic, financial, language, and time. These aren't excuses, just realities that the good folks @ASNKidney are trying to overcome to achieve parity in the membership roll.
11/#rpa21
But in #KidneyWk, there are no geographic, financial, language, or time barriers...yet the growth rate of female scientists is identical to that of the @ASNKidney membership roll: ~1% per year.
This is a true *underperformance* in gender representation in #kidneyWk
But in #KidneyWk, there are no geographic, financial, language, or time barriers...yet the growth rate of female scientists is identical to that of the @ASNKidney membership roll: ~1% per year.
This is a true *underperformance* in gender representation in #kidneyWk
12/#rpa21
If *representation* is having a seat at the table, then *inclusion* is having a voice at that table.
Shown here is the slow but steady increase in female speakers, moderators, program chairs at the @ASNKidney annual meeting. Growth is slow, but present.
If *representation* is having a seat at the table, then *inclusion* is having a voice at that table.
Shown here is the slow but steady increase in female speakers, moderators, program chairs at the @ASNKidney annual meeting. Growth is slow, but present.

13/#rpa21
Inclusion in #KidneyWk, however, is a somewhat better story. First, let's understand how inclusion is measured in an online community.
One's *voice* manifests in the number of tweets s/he composes. Shown here are the number of tweets by gender from 2011 to 2020.
Inclusion in #KidneyWk, however, is a somewhat better story. First, let's understand how inclusion is measured in an online community.
One's *voice* manifests in the number of tweets s/he composes. Shown here are the number of tweets by gender from 2011 to 2020.
14/#rpa21
Key points in this bar chart:
a)the first nephrology conference on Twitter was #kidneyWk in 2011, where female scientists had a greater voice than male counterparts (6.2 v 4.3)
b)After this initial success, the female voice drops for the next 5 years (2012-2016).......
Key points in this bar chart:
a)the first nephrology conference on Twitter was #kidneyWk in 2011, where female scientists had a greater voice than male counterparts (6.2 v 4.3)
b)After this initial success, the female voice drops for the next 5 years (2012-2016).......

15/#rpa21
c)it's not until 2017 that we see near parity of female inclusion and then a greater female voice in 2020 (pandemic) compared to male counterparts.
Glad to see female inclusion reaching/exceeding the male voice, but don't want to see the pattern of 2011 repeat.
c)it's not until 2017 that we see near parity of female inclusion and then a greater female voice in 2020 (pandemic) compared to male counterparts.
Glad to see female inclusion reaching/exceeding the male voice, but don't want to see the pattern of 2011 repeat.

16/#rpa21
*Belonging is having your voice heard.
Many ways to measure it: at @NODanalytics we measure belonging by measuring *intent*.
If a scientist wants to communicate with someone, s/he will make her/his intent known in their tweet.
*Belonging is having your voice heard.
Many ways to measure it: at @NODanalytics we measure belonging by measuring *intent*.
If a scientist wants to communicate with someone, s/he will make her/his intent known in their tweet.

17/#rpa21
Shown here: scientists who made their intent known to communicate with a male (dark blue) or female (mahogany red) scientist @ #kidneywk.
Male and female scientists are 3x and 2x (respectively) less likely to communicate w/a female scientist than a male (2015-2020).
Shown here: scientists who made their intent known to communicate with a male (dark blue) or female (mahogany red) scientist @ #kidneywk.
Male and female scientists are 3x and 2x (respectively) less likely to communicate w/a female scientist than a male (2015-2020).

18/#rpa21
Our challenge to achieve gender equality:
•Increase representation at a faster rate than seen in the @ASNKidney membership data
•Maintain female inclusion & avoid a repeat of the pattern first seen in 2011
•Increase female belonging among male & female scientists
Our challenge to achieve gender equality:
•Increase representation at a faster rate than seen in the @ASNKidney membership data
•Maintain female inclusion & avoid a repeat of the pattern first seen in 2011
•Increase female belonging among male & female scientists

19/#rpa21
Challenge #2: Polarization
All groups (live or online) are going to be polarized.
In the real world, the same barriers that slow our efforts to achieve gender equality also result in polarization: geography, language, finances, and time.
Challenge #2: Polarization
All groups (live or online) are going to be polarized.
In the real world, the same barriers that slow our efforts to achieve gender equality also result in polarization: geography, language, finances, and time.

20/#rpa21
None of these barriers exist online, so why do we have polarization? Algorithmic design.
@pewresearch has defined 6 Twitter morphologies: all have some degree of polarization, but extremely polarized groups slow the sharing of science, among other detriments.
None of these barriers exist online, so why do we have polarization? Algorithmic design.
@pewresearch has defined 6 Twitter morphologies: all have some degree of polarization, but extremely polarized groups slow the sharing of science, among other detriments.

21/#rpa21
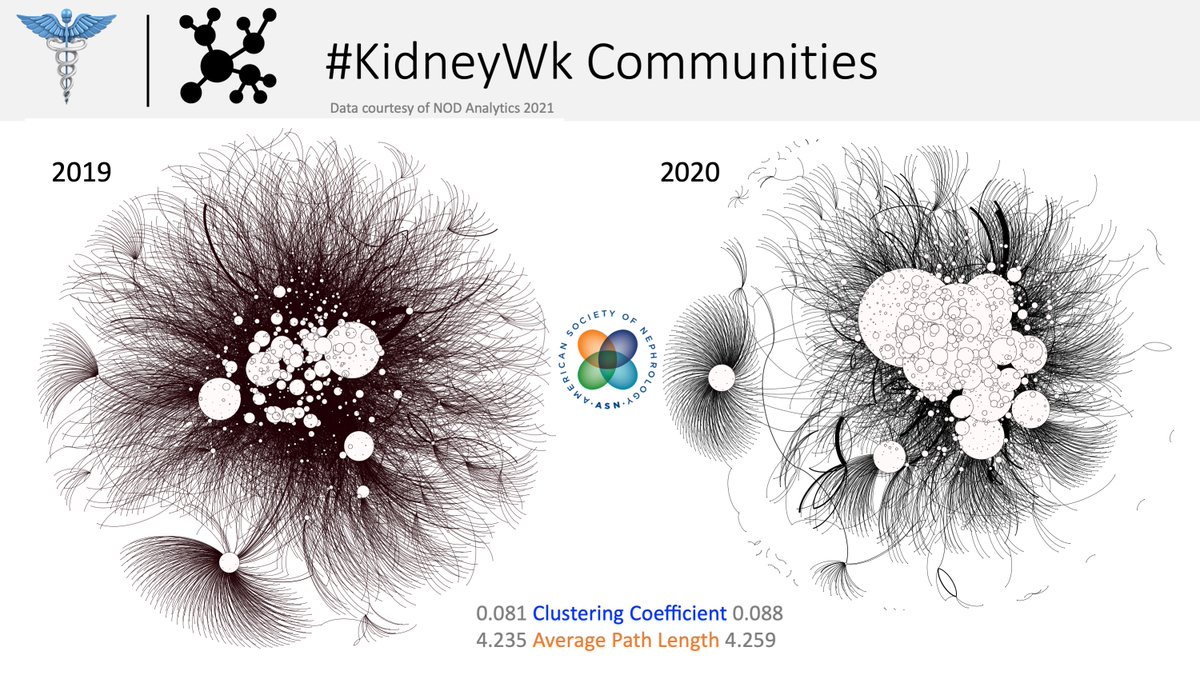
We can both measure and visualize polarization. We will analyze the Twitter networks of @ASNKidney, @ERAEDTA, and @NKF_NephPros.
We'll use two metrics:
Clustering Coefficient: from 0 to 1. Higher means less polarization
APL: Lower means less polarization
We can both measure and visualize polarization. We will analyze the Twitter networks of @ASNKidney, @ERAEDTA, and @NKF_NephPros.
We'll use two metrics:
Clustering Coefficient: from 0 to 1. Higher means less polarization
APL: Lower means less polarization

22/#rpa21
Left graph shows the entire #KidneyWk network for 2019 (brown) & 2020 (black). Clustering Coefficient & Average Path Length barely rise.
Right graph: the CC and APL trends since 2016: both metrics are trending towards more polarization in #kidneyWk as the years go by.
Left graph shows the entire #KidneyWk network for 2019 (brown) & 2020 (black). Clustering Coefficient & Average Path Length barely rise.
Right graph: the CC and APL trends since 2016: both metrics are trending towards more polarization in #kidneyWk as the years go by.

23/#rpa21
We've measured polarization..now let's visualize it.
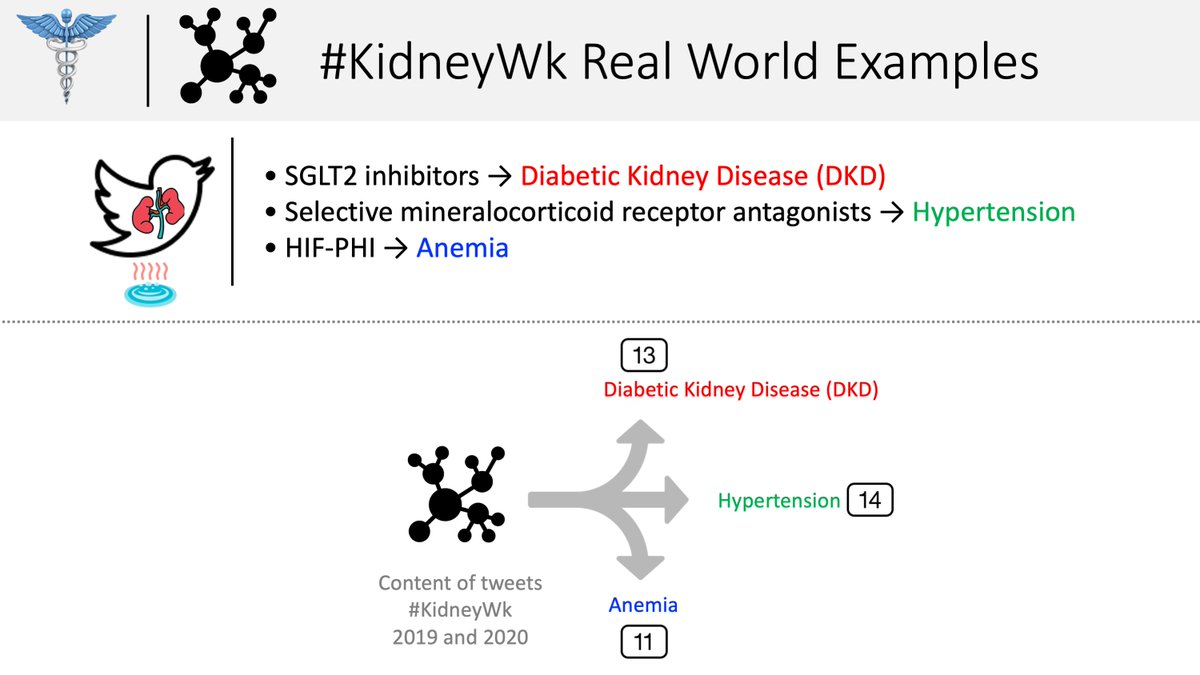
We'll look at tweet content in #KidneyWk 2019 and 2020 of 3 hot topics:
SGLT2i: incorporated into a package of 13 terms related to DKD
Selective MRAs → 14 terms related to HTN
HIF-PHI → 11 terms related to anemia
We've measured polarization..now let's visualize it.
We'll look at tweet content in #KidneyWk 2019 and 2020 of 3 hot topics:
SGLT2i: incorporated into a package of 13 terms related to DKD
Selective MRAs → 14 terms related to HTN
HIF-PHI → 11 terms related to anemia
24/#rpa21
Left: 2019 #KidneyWk in brown with red lines indicating sharing of information related to DKD.
Right: 2020 in black; all else as above.
Zoom in on the graphs and you can see whole chunks of #NephTwitter people who receive no info about DKD.
That's polarization (bad).
Left: 2019 #KidneyWk in brown with red lines indicating sharing of information related to DKD.
Right: 2020 in black; all else as above.
Zoom in on the graphs and you can see whole chunks of #NephTwitter people who receive no info about DKD.
That's polarization (bad).


25/#rpa21
Same idea as above, this time for hypertension.
Q: What type of scientific discourse will scientists have with each other if one is completely polarized and receives no information about hypertension.
A: No common set of shared facts upon which consensus can be built
Same idea as above, this time for hypertension.
Q: What type of scientific discourse will scientists have with each other if one is completely polarized and receives no information about hypertension.
A: No common set of shared facts upon which consensus can be built


26/#rpa21
Shown here is anemia.
Without a shared set of facts, we cannot reach consensus, or having meaningful scientific discourse. This is what polarization looks like...and if you think you aren't locked into a polarized group...well, that's what the algorithms want u to think
Shown here is anemia.
Without a shared set of facts, we cannot reach consensus, or having meaningful scientific discourse. This is what polarization looks like...and if you think you aren't locked into a polarized group...well, that's what the algorithms want u to think


27/#rpa21
But..#KidneyWk is going to be polarized because it's the largest Nephrology meeting on Twitter. Polarization is a natural consequence of large networks, right?
Let's compare the @ASNKidney online network with those from @ERAEDTA and @NKF_NephPros from 2016 to 2020.
But..#KidneyWk is going to be polarized because it's the largest Nephrology meeting on Twitter. Polarization is a natural consequence of large networks, right?
Let's compare the @ASNKidney online network with those from @ERAEDTA and @NKF_NephPros from 2016 to 2020.

28/#rpa21
Shown here are the clustering coefficients (blue) and APL (orange) for @ASNKidney @NKF_NephPros & @ERAEDTA meetings (respectively)
Above each graph is the Pearson coefficient of the CC and number of people (network size) or APL and network size.
Shown here are the clustering coefficients (blue) and APL (orange) for @ASNKidney @NKF_NephPros & @ERAEDTA meetings (respectively)
Above each graph is the Pearson coefficient of the CC and number of people (network size) or APL and network size.

29/#rpa21
CC & network size: @ERAEDTA is 0.9, suggesting that network size does *not* result in polarization.
APL & network size: as the @ERAEDTA network size increases, they're able to decrease polarization
@NKF_NephPros shows similar trends but not the @ASNKidney #KidneyWk
CC & network size: @ERAEDTA is 0.9, suggesting that network size does *not* result in polarization.
APL & network size: as the @ERAEDTA network size increases, they're able to decrease polarization
@NKF_NephPros shows similar trends but not the @ASNKidney #KidneyWk

30/#RPA21
So our challenge with polarized networks:
Polarization is not related to network size, so this isn't a "necessary evil" or the price we pay for having a popular #nephTwitter network.
How does @ERAEDTA & @NKF_NephPros dissociate size & polarization? Can it be replicated?
So our challenge with polarized networks:
Polarization is not related to network size, so this isn't a "necessary evil" or the price we pay for having a popular #nephTwitter network.
How does @ERAEDTA & @NKF_NephPros dissociate size & polarization? Can it be replicated?

31/#RPA21
The last challenge: the perils of customized search.
How could anything that is customized be a bad thing?
Everyone has to pay the same price when they're given something customized: awareness
A lack of awareness is deleterious to scientific discourse.
The last challenge: the perils of customized search.
How could anything that is customized be a bad thing?
Everyone has to pay the same price when they're given something customized: awareness
A lack of awareness is deleterious to scientific discourse.

32/#RPA21
What's the difference between a customized & standard search?
Standard: your search query determines the results you see and the hierarchy of those results
Customized: your search query is passed through an algorithm-influenced filter and sorter...
What's the difference between a customized & standard search?
Standard: your search query determines the results you see and the hierarchy of those results
Customized: your search query is passed through an algorithm-influenced filter and sorter...

33/#RPA21
Algorithms use your previous behaviors (RTs ❤️💬) to present unique results in a distinct rank order. Why?
The goal is to encourage said behavior.
So 2 scientists searching the same thing will be presented with a different set of facts, hurting scientific discourse.
Algorithms use your previous behaviors (RTs ❤️💬) to present unique results in a distinct rank order. Why?
The goal is to encourage said behavior.
So 2 scientists searching the same thing will be presented with a different set of facts, hurting scientific discourse.

34/#RPA21
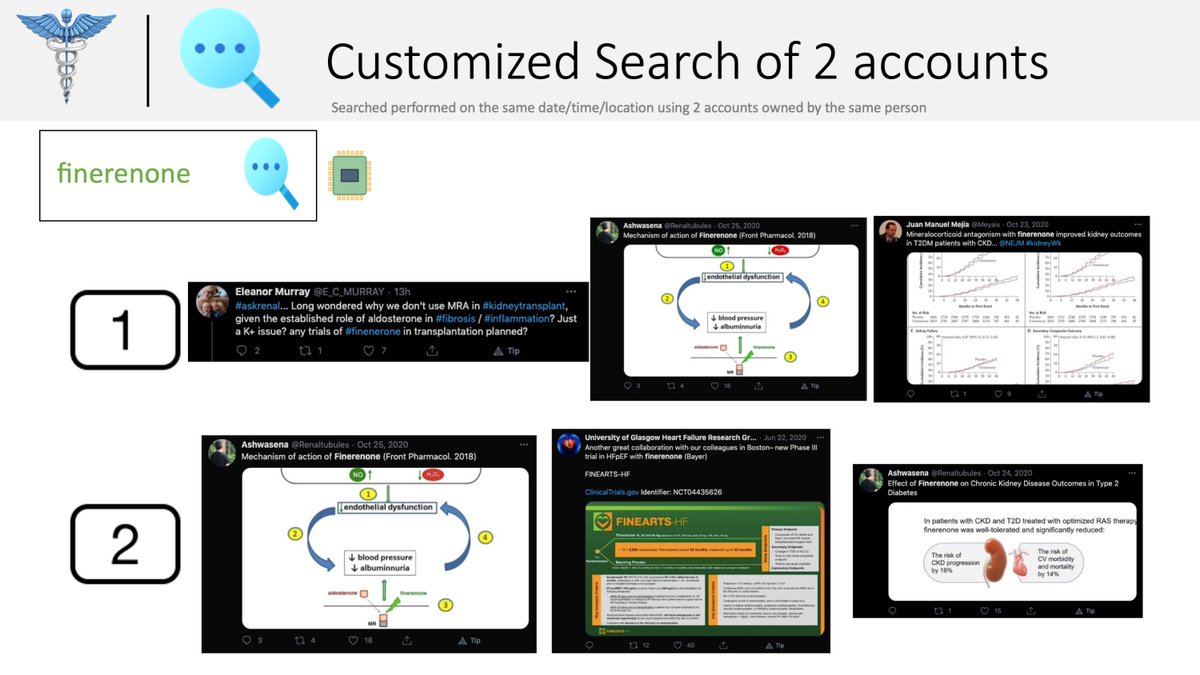
These slides show customized search in action.
I own both accounts & searched the same terms using the same syntax, at the same date and time (2 seconds apart), from the same location.
The same (owner, query, syntax, date/time, location) →→→ different results
These slides show customized search in action.
I own both accounts & searched the same terms using the same syntax, at the same date and time (2 seconds apart), from the same location.
The same (owner, query, syntax, date/time, location) →→→ different results

35/#RPA21
The challenge: neutralizing algorithms that use our previous behavior to display search results whose goal is to reinforce that behavior.
How can scientists implement standard search to get the same results in the same order in order to share a common set of facts?
The challenge: neutralizing algorithms that use our previous behavior to display search results whose goal is to reinforce that behavior.
How can scientists implement standard search to get the same results in the same order in order to share a common set of facts?

36/#RPA21
Solution time.
Our first challenge to overcome is the gender inequality in #nephTwitter.
Identify yourself
Make public Twitter lists (an online rolodex)
Tweet with intent & not into the cyber-abyss
Solution time.
Our first challenge to overcome is the gender inequality in #nephTwitter.
Identify yourself
Make public Twitter lists (an online rolodex)
Tweet with intent & not into the cyber-abyss

37/#RPA21
Second challenge: polarized networks and their corrupt influence on scientific discourse.
The most important thing: take a page out of #OncTwitter's playbook & standardize disease-specific hashtags to break out of one's polarized group.
Second challenge: polarized networks and their corrupt influence on scientific discourse.
The most important thing: take a page out of #OncTwitter's playbook & standardize disease-specific hashtags to break out of one's polarized group.

38/#RPA21
Third challenge: use standard search to ensure that the results you see allow you to have a shared set of facts with others.
Use a standard Twitter search engine: NephTwitterArchive.com
It's bias-free and works: 1345 searches completed per month since 10/2019
Third challenge: use standard search to ensure that the results you see allow you to have a shared set of facts with others.
Use a standard Twitter search engine: NephTwitterArchive.com
It's bias-free and works: 1345 searches completed per month since 10/2019

39/#RPA21
Don't ignore these challenges because they are already decreasing the value of our #nephTwitter communities.
Reach out to me if you need further clarification.
Thanks and good luck in making a better Twitter learning environment and improve the scientific discourse.
Don't ignore these challenges because they are already decreasing the value of our #nephTwitter communities.
Reach out to me if you need further clarification.
Thanks and good luck in making a better Twitter learning environment and improve the scientific discourse.


• • •
Missing some Tweet in this thread? You can try to
force a refresh