
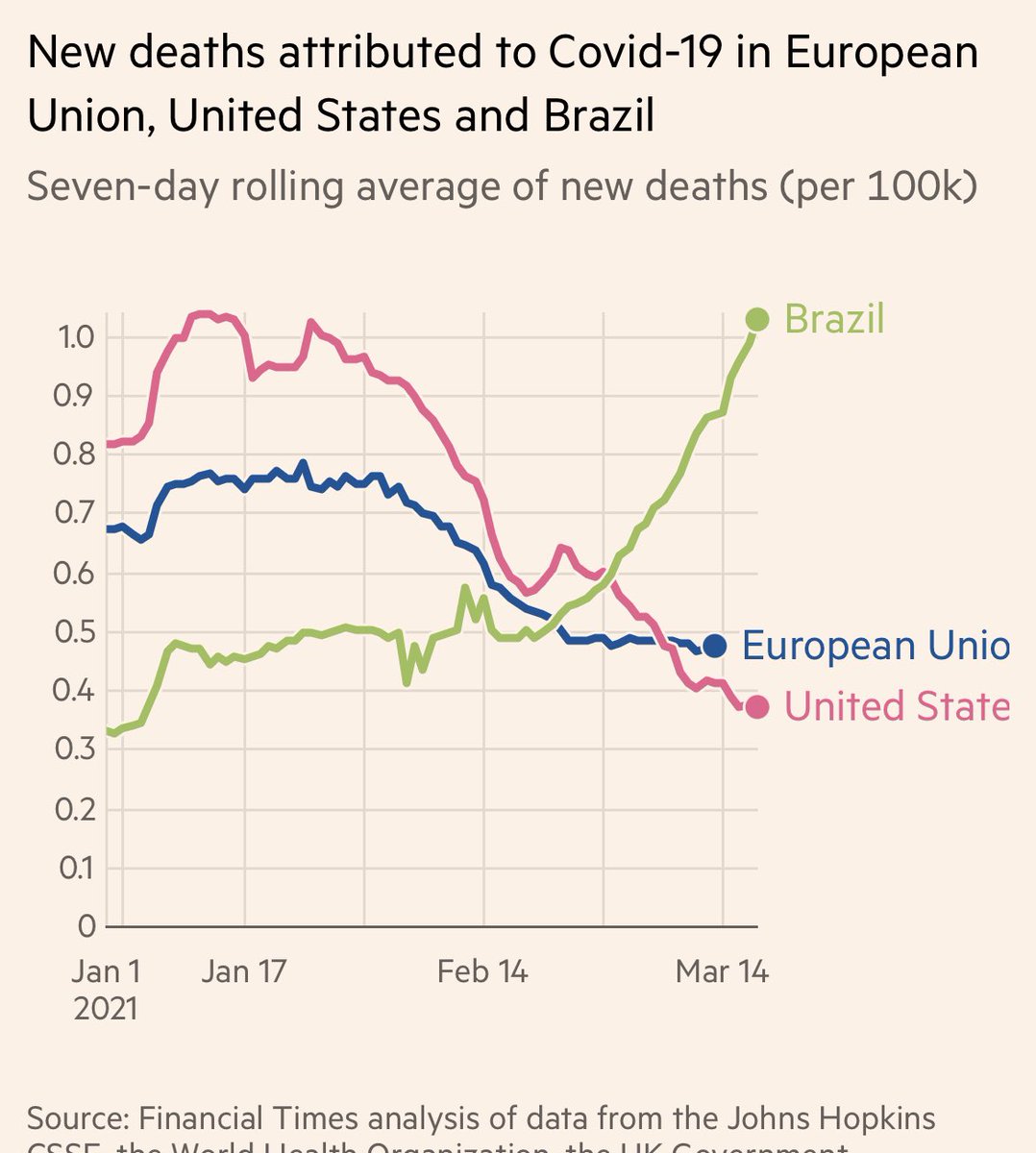
PAY ATTENTION—There is one crisis we all needs to pay attention to—and that is the unprecedented Brazil 🇧🇷 surge of the #P1 variant, overloaded hospitals, & sharp mortality spike. If more contagious #P1 out of control worldwide, we are all endangered. 🧵
#SOSBrazil #COVID19
#SOSBrazil #COVID19
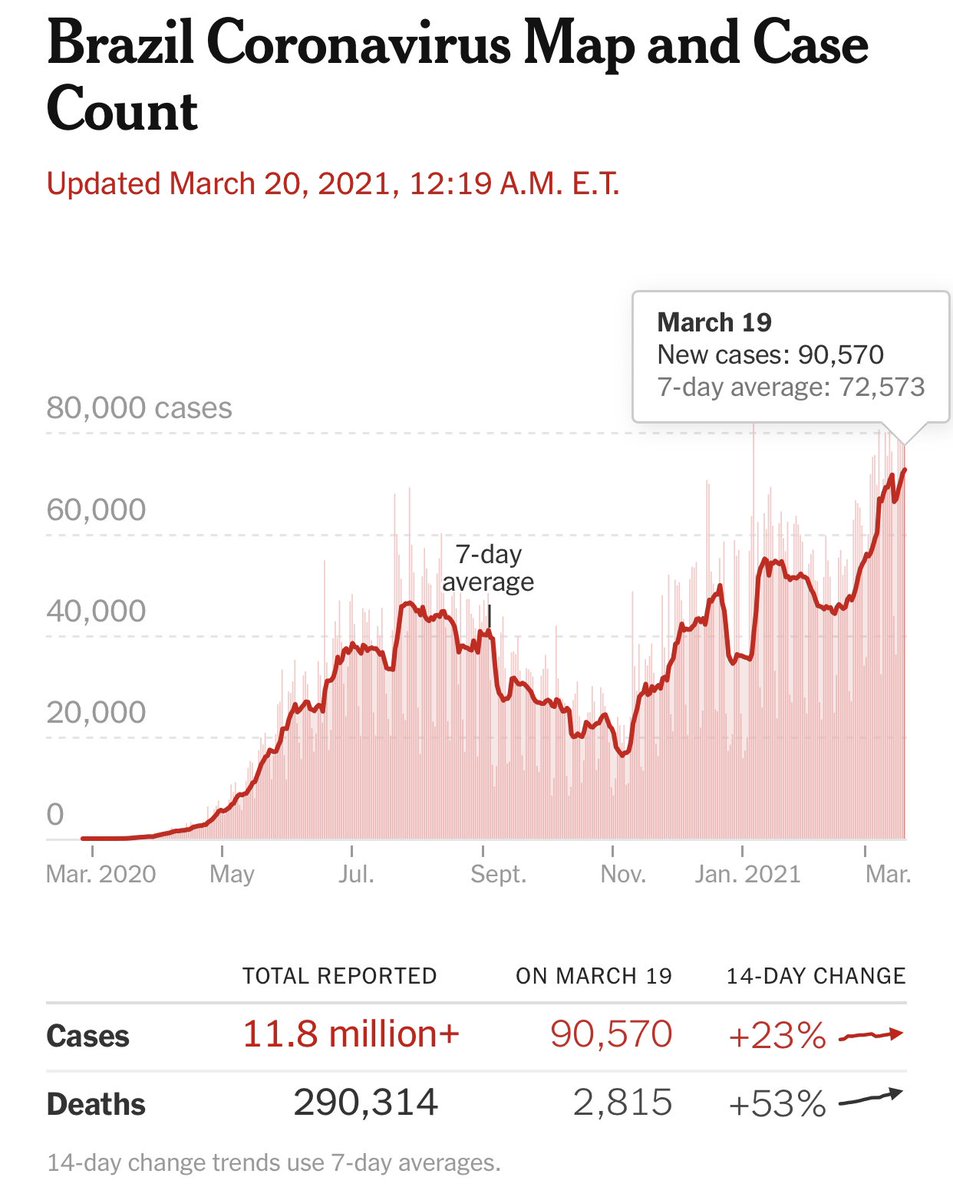
2) I cannot overemphasis how serious the crisis in Brazil is. It is virtually impossible to find any ICU bed, and many hospitals running out of sedative medications to perform intubation with—so doctors are intubating without any analgesic meds. Hospitals are in collapse.
https://twitter.com/DrEricDing/status/1372005826383204353
3) I’m not exaggerating that hospitals in Brazil are in collapse. This is the headline of a major newspaper.

4) Don’t just listen to me. Listen to the reporting on the ground. This report was filed last week by @MattRiversCNN — he says it has gotten only worse.
https://twitter.com/drericding/status/1372305355460517891?s=10
5) Nobody can deny the pandemic when hospitals are completely overrun. Don’t let anyone dismiss #COVID19 and what is happening in Brazil - hospitalizations and deaths DO NOT LIE.

6) The crisis is described by the @fiocruz @fiocruz_en foundation as the **worst sanitation and hospital collapse in the history of Brazil**

7) I’m told by reporters that even “we're also hearing very consistently, that in Brazil more and more young people are dying on the virus. doctors keep telling us that their patients keep getting younger, no comorbidities” - from doctors across many cities. @MattRiversCNN
8) But also more concerning — Brazil experts analysis says P1 is potentially 2-2.5x faster transmission (more contagious) than the old common strains. That means it is also faster than #B117 sweeping the world.
We need to get serious about Brazil crisis.
We need to get serious about Brazil crisis.
https://twitter.com/drericding/status/1372013248980074498?
9) Another Brazil research group puts #P1 transmission at 2x faster than old strain (instead of 2.5x above), but they estimate a way worse whopping 25-60% reinfection rate. That’s serious.
bbc.com/news/amp/healt…
bbc.com/news/amp/healt…

10) How good is are the mRNA vaccines against this #P1 variant menace? Only semi— it has moderate neutralization- better than the SA #B1351, but worse than #B117 (which responds well to vaccine).
FYI earlier Pfizer-conducted study said okay, but this bigger study disagrees.
FYI earlier Pfizer-conducted study said okay, but this bigger study disagrees.
https://twitter.com/DrEricDing/status/1371209487491735553
11) But the problem for Brazil is that it doesn’t have the mRNA vaccines. It has the AstraZeneca and SinoVac vaccine. We don’t know the exact efficacy yet for #P1, but SinoVac vaccine showed a much lower 50% efficacy in Brazil trials, before P1.
google.com/amp/s/www.bbc.…
google.com/amp/s/www.bbc.…
12) Now 50% is still good, and for severe disease, it’s 78% for SinoVac, so that’s decent.
J&J vaccine shows mid to upper 80% for Brazil, but J&J isn’t available in Brazil yet either.
Main problem is Brazil doesn’t have enough! google.com/amp/s/amp.cnn.…
J&J vaccine shows mid to upper 80% for Brazil, but J&J isn’t available in Brazil yet either.
Main problem is Brazil doesn’t have enough! google.com/amp/s/amp.cnn.…
13) state of Rio de Janeiro suspended its vaccination campaign because it had run out of vaccine supplies.
"This is a disaster, a total disaster," a woman told CNN after being denied her vaccine. "Who is to blame for all this? I think our leaders, our politicians suck."
"This is a disaster, a total disaster," a woman told CNN after being denied her vaccine. "Who is to blame for all this? I think our leaders, our politicians suck."
14) “less than 10 million people in the country of about 220 million had received at least one dose, according to federal health data. Only 1.57% of the population had been fully vaccinated.”
THIS IS AN EPIC DISASTER in the making for Brazil. google.com/amp/s/amp.cnn.…
THIS IS AN EPIC DISASTER in the making for Brazil. google.com/amp/s/amp.cnn.…
15) How the hell did Brazil screw up its vaccine supply so much?
“multiple experts say the ineptitude of the federal government, led by Covid-skeptic Bolsonaro, has sabotaged. They point to a distinct lack of urgency on the fed govt to secure supplies”
cnn.com/2021/02/01/ame…
“multiple experts say the ineptitude of the federal government, led by Covid-skeptic Bolsonaro, has sabotaged. They point to a distinct lack of urgency on the fed govt to secure supplies”
cnn.com/2021/02/01/ame…
16) Brazil is in talks with the US to import some vaccines. The US already “loaned” 4 million doses to Mexico & Canada. But the talks with Brazil started March 13th and still have not reached any deal. Brazil needs it soon. Hope Bolsonaro is playing ball.
google.com/amp/s/www.voan…
google.com/amp/s/www.voan…
17) Even with vaccine imports, and the delay in rollout and immunity kicking in, the next month will be brutal for Brazil. We might see what unmitigated full onslaught with a downplaying Bolsonaro looks like.
Meantime, Brazil ordering 3x the coffins.
metropoles.com/brasil/covid-a…
Meantime, Brazil ordering 3x the coffins.
metropoles.com/brasil/covid-a…
18) But I also want to offer a message of hope to the people of Brazil 🇧🇷— the world sees your struggle and your pain. I talk to colleagues at the WHO and in DC. The world has not forgotten you—even if your leader maybe sometimes has. The world needs to care and does care.
19) Meantime, Bolsonaro is the one person that world leaders need to call out and pressure. He is literally stopping all efforts to improve the situation. This is untenable.
If this Brazil crisis keeps going, I worry for its stability. google.com/amp/s/amp.cnn.…
If this Brazil crisis keeps going, I worry for its stability. google.com/amp/s/amp.cnn.…

20) I don’t believe in doomed fate. “There is no fate but what we make.”
Brazil needs help, Brazil needs change. Brazil needs leadership that will put human lives first, and to end suffering of its poor.
May God & the world help the people of Brazil.
Brazil needs help, Brazil needs change. Brazil needs leadership that will put human lives first, and to end suffering of its poor.
May God & the world help the people of Brazil.
21) To the rest of the 🌎—please don’t be selfishly withholding aid/vaccines. If Brazil’s #P1 crisis grows, so will the risk for the world. We rise as fall as one planet & civilization. We need to remember the motto—“All for one, one for all”—let’s all find our inner humanity. 🙏
22) p.s. the Oxford-AstraZeneca reported to be is efficacious against the #P1 variant. But the study hasn’t be released yet by researchers - details forthcoming.
US has a stockpile over over 30 million doses of AstraZeneca—it needs to release now.
cnbc.com/2021/03/05/oxf…
US has a stockpile over over 30 million doses of AstraZeneca—it needs to release now.
cnbc.com/2021/03/05/oxf…
23) UK Imperial team:
⚠️“data show #P1 variant is 1.4-2.2 times more transmissible than other variants & original #SARSCoV2 strain, and 25%-65% more likely to evade existing protective immunity from previous non-P.1 infections—susceptible to reinfection.”
edition.cnn.com/world/live-new…
⚠️“data show #P1 variant is 1.4-2.2 times more transmissible than other variants & original #SARSCoV2 strain, and 25%-65% more likely to evade existing protective immunity from previous non-P.1 infections—susceptible to reinfection.”
edition.cnn.com/world/live-new…

24) The catastrophe in Brazil is the worst in its history. And likely will be the worst in the annals of this pandemic — we desperately need to urgently send aid and vaccines to Brazil 🇧🇷.
Please help @WHCOS @aslavitt46 @ASlavitt @JeffZients @DrTedros @mvankerkhove @gabbystern
Please help @WHCOS @aslavitt46 @ASlavitt @JeffZients @DrTedros @mvankerkhove @gabbystern
https://twitter.com/DrEricDing/status/1373690086831841287
25) good news - vaccine deals inked by Brazil to buy more.
Bad news—most of the vaccines ordered aren’t coming for many many months.
Bad news—most of the vaccines ordered aren’t coming for many many months.
https://twitter.com/DrEricDing/status/1373708522928635911
26) Vaccine inequality is the great inequality that will lead to more tragedy in this pandemic.
We need to send vaccines urgently to Brazil, Mexico, and all of Latin America. #COVID19 #COVID19Vaccine
(HT @fibke)
We need to send vaccines urgently to Brazil, Mexico, and all of Latin America. #COVID19 #COVID19Vaccine
(HT @fibke)

27) The longer we neglect to vaccinate low and middle income countries (LMIC), the longer this crisis will continue.
#VaccinEquity for Brazil and all of Latin America and Africa and Asia.
(Ht @fibke)
pandem-ic.com/vaccine-equity…
#VaccinEquity for Brazil and all of Latin America and Africa and Asia.
(Ht @fibke)
pandem-ic.com/vaccine-equity…

28) ...I’m hearing some signals US might help Brazil hospitals in some potential ways soon. Unclear what yet. But there are some in WH that are exploring. Fingers crossed of what’s to come.
29) this was Brazil 3 days ago... and those spikes have now surged even more.
https://twitter.com/DGBassani/status/1374565615172739073
30) Now Brazil’s #P1 crisis has spilled over into neighboring countries...
https://twitter.com/DrEricDing/status/1375274363843444742
31) And now #P1 has invaded North America - British Columbia 🇨🇦 has a recent sudden surge of #P1.
https://twitter.com/DrEricDing/status/1375617997046435845
32) The Brazilian 🇧🇷 #P1 epidemic has now definitively spilled into other countries and caused outbreaks—the largest being in British Columbia, Canada.
https://twitter.com/DrEricDing/status/1377819829466464258
33) P.s. small update on Brazil 🇧🇷 situation - I have receive word that Brazil is now engaging with the US directly. Hopeful 🙏
34) Brazil needs to act fast.... now more young people are dying than in first wave.
https://twitter.com/DrEricDing/status/1375982129331511299
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















