
The #Brisbane outbreak is the result of incompetence.
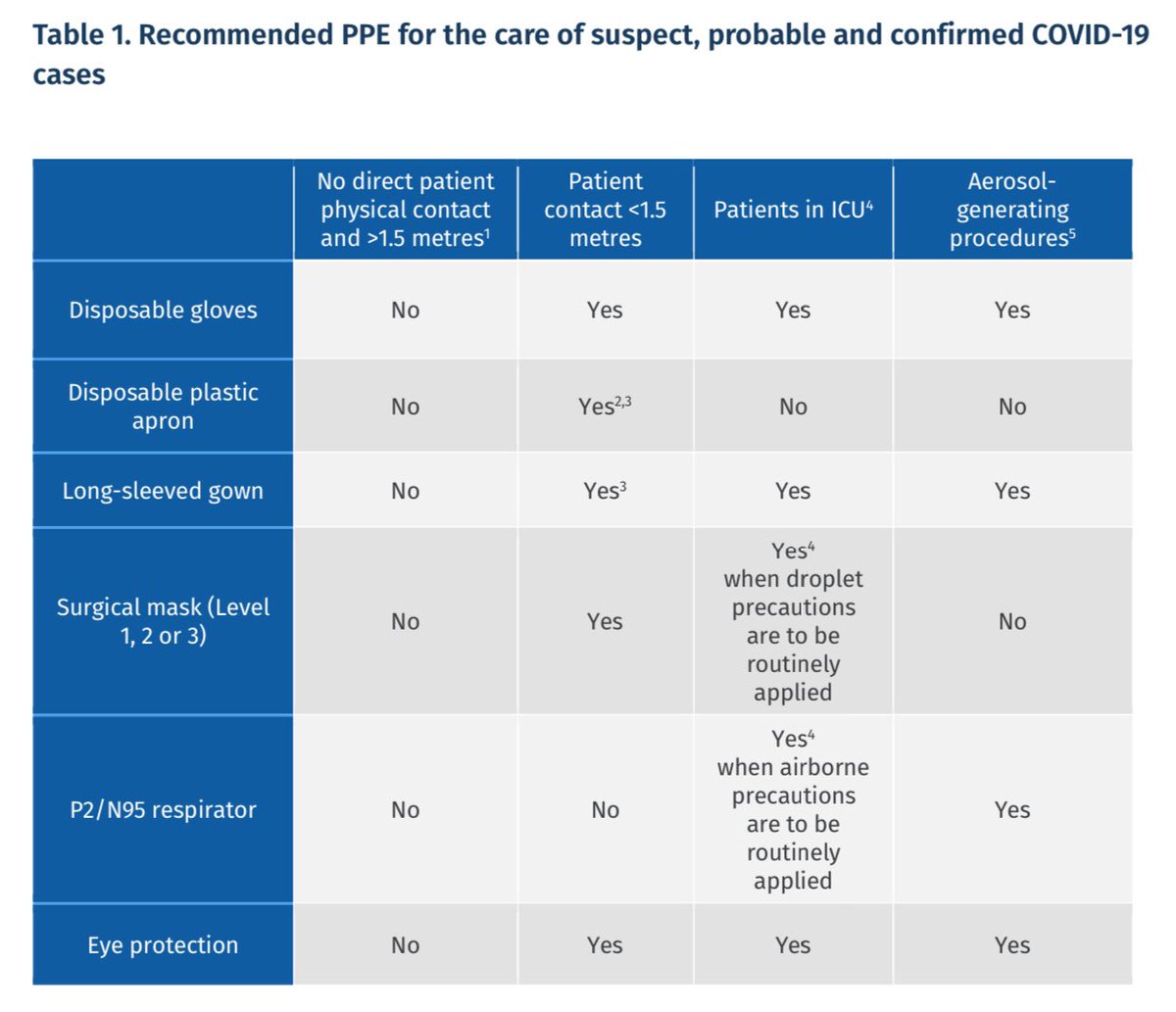
Doctors aren’t getting airborne PPE (P2/N95 respirators). If distance can be maintained, masks aren’t required at all!
SARS-CoV-2 is airborne, so why is Queensland following substandard guidance?
#BrisbaneLockdown #auspol
Doctors aren’t getting airborne PPE (P2/N95 respirators). If distance can be maintained, masks aren’t required at all!
SARS-CoV-2 is airborne, so why is Queensland following substandard guidance?
#BrisbaneLockdown #auspol
https://twitter.com/bnodesk/status/1376301929681276931

Additionally, the doctor at the centre of the Brisbane outbreak should have been vaccinated.
Currently, the greatest risk to Australia comes from overseas arrivals. We need to put a protective ring around the quarantine system, by vaccinating these Australian workers first.
Currently, the greatest risk to Australia comes from overseas arrivals. We need to put a protective ring around the quarantine system, by vaccinating these Australian workers first.
Here’s a link to the infection control guidelines for Queensland.
Healthcare workers are routinely given inadequate protection - or perhaps no protection at all, if distance can be maintained!
This is inadequate for an airborne virus like SARS-CoV-2.
health.qld.gov.au/__data/assets/…
Healthcare workers are routinely given inadequate protection - or perhaps no protection at all, if distance can be maintained!
This is inadequate for an airborne virus like SARS-CoV-2.
health.qld.gov.au/__data/assets/…
There are numerous documented examples of outbreaks caused by airborne transmission around the world.
Here’s an example of airborne transmission from South Korea:
Here’s an example of airborne transmission from South Korea:
https://twitter.com/drzoehyde/status/1341317707690463232?s=21
Another example of airborne transmission from South Korea:
https://twitter.com/drzoehyde/status/1334174667536355330?s=21
Another example of airborne transmission from New Zealand:
https://twitter.com/drzoehyde/status/1372879980921647106?s=21
Another example of airborne transmission from Israel:
https://twitter.com/drzoehyde/status/1355780619238662146?s=21
Another example of airborne transmission from the USA:
https://twitter.com/drzoehyde/status/1370675383872278532?s=21
Another example of airborne transmission from China:
https://twitter.com/DrZoeHyde/status/1305408228147097600
• • •
Missing some Tweet in this thread? You can try to
force a refresh










