Today it’s Lung #POCUS for you!
It is:
Easy to perform
Accurate
Sensitive
Repeatable
Negates irradiation or transport elsewhere!
#FOAMed #POCUS #FOAMcc #foamus @icmteaching @ICUltrasonica
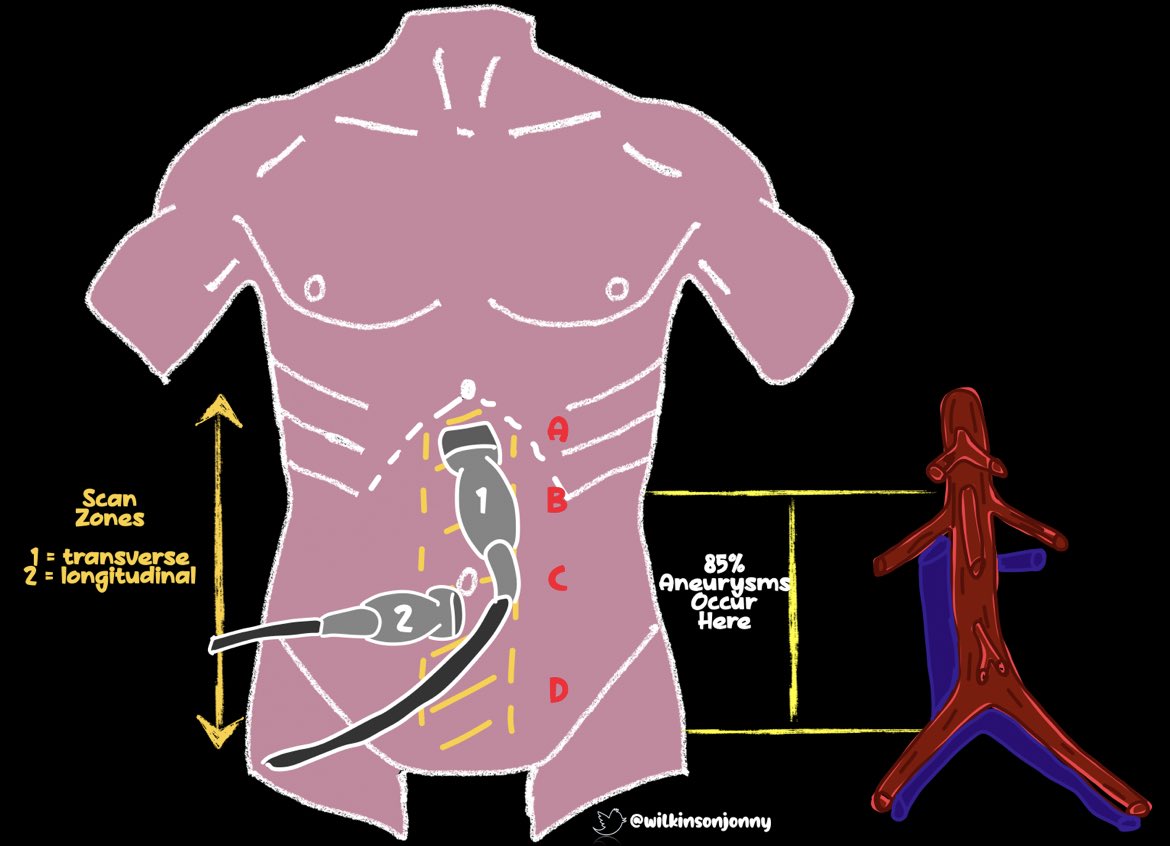
Where do we scan then?? Linear/curvilinear or phased probe positions shown👍👇
It is:
Easy to perform
Accurate
Sensitive
Repeatable
Negates irradiation or transport elsewhere!
#FOAMed #POCUS #FOAMcc #foamus @icmteaching @ICUltrasonica
Where do we scan then?? Linear/curvilinear or phased probe positions shown👍👇
We don’t tend to use linear for the basal sections, as you need depth for the PLAPS points. To see the pleura clearly, minimise depth and drop gain down, you get a real concept of sliding on the screen.
Here are the normal views for you @GEHealthcare
Here are the normal views for you @GEHealthcare
Now; the Pneumothorax!
Pleural slide disappears as the parietal and visceral pleura separate. So, a static washing line is seen between the rib pillars 👇. The more you see, the more you recognise. Decompress IF your patient is compromised. It’s more sensitive than CXR!
Pleural slide disappears as the parietal and visceral pleura separate. So, a static washing line is seen between the rib pillars 👇. The more you see, the more you recognise. Decompress IF your patient is compromised. It’s more sensitive than CXR!
Here is another view with a linear probe. The pleura is visualised better with the high frequency probe.
Now here, we can see the lung point, where non-sliding meets sliding pleura. Very sensitive for PTX.
If you see this, you can hand on heart diagnose PTX!
Now here, we can see the lung point, where non-sliding meets sliding pleura. Very sensitive for PTX.
If you see this, you can hand on heart diagnose PTX!
Even more lung point action on this scan series.
We have multiple intercostal spaces here, and you see where the PTX appears!
-@GEHealthcare now have the fabulous lung sweep available to do this for you! Fantastic stuff:
pocushub.net/npi/critical-m…
We have multiple intercostal spaces here, and you see where the PTX appears!
-@GEHealthcare now have the fabulous lung sweep available to do this for you! Fantastic stuff:
pocushub.net/npi/critical-m…
If you are unsure if slide is there or not, place m-mode down through the rib window. If you see a seashore appearance, the slide has created the Sandy beach interference.
If there’s no sliding, you get a barcode or stratosphere sign as below. You’ve backed up your diagnosis!
If there’s no sliding, you get a barcode or stratosphere sign as below. You’ve backed up your diagnosis!
Now; if we intubate the right main bronchus, there is little to no slide on the left🤷♂️
But - it’s not a PTX. If we shine m-mode through, we will get a lung pulse.
This is where cardiac pulsation is amplified via opposed intact pleura giving us a blip in unison with the pulse👍
But - it’s not a PTX. If we shine m-mode through, we will get a lung pulse.
This is where cardiac pulsation is amplified via opposed intact pleura giving us a blip in unison with the pulse👍
Now, interstitial fluid!
Fluid allows sound waves to travel through. We see this as beams travelling from the pleura right to the bottom of the image. These are b-lines. The more there are, the ‘wetter’ the lungs.
Diuresis can help / fluid restriction. It could be #COVID19 too.
Fluid allows sound waves to travel through. We see this as beams travelling from the pleura right to the bottom of the image. These are b-lines. The more there are, the ‘wetter’ the lungs.
Diuresis can help / fluid restriction. It could be #COVID19 too.
Here is another, but in this one, we see spared areas of normal lung and visible horizontal a-lines.
B-lines are vertical remember.
A = ‘A-cross’
B = to the ‘B-ottom’
B-lines are vertical remember.
A = ‘A-cross’
B = to the ‘B-ottom’
Now; in #COVID19 we get a pneumonitis. And hence, fluid in the form of B-lines.
Classically, we see jagged and thickened pleura too. So, test positive and this US appearance is typical! So much more sensitive than CXR!
Classically, we see jagged and thickened pleura too. So, test positive and this US appearance is typical! So much more sensitive than CXR!
Here’s another #COVID19 view. This patient’s hypoxia was aided by CPAP and diuretics. More B’s = more fluid!
You can often see subtler US changes well before any CXR flags it. And forget the stethoscope when you have US!
B-lines often clear with good diuresis.
You can often see subtler US changes well before any CXR flags it. And forget the stethoscope when you have US!
B-lines often clear with good diuresis.
What about consolidation?
Eminently detectable with lung #POCUS !
Here we see white shred appearance of consolidation. The shred describes where infected lung interfaces with normal lung.
Eminently detectable with lung #POCUS !
Here we see white shred appearance of consolidation. The shred describes where infected lung interfaces with normal lung.
And some more consolidation. Normal lung is air filled and appears black.
The more abnormal echogenic specs there are, the more consolidation is forming.
The more abnormal echogenic specs there are, the more consolidation is forming.
Here’s another example of consolidation in #COVID19, with a small parapnemonic effusion.
We saw a lot of superadded bacterial infections in COVID. You don’t classically see straight forward consolidation with simple viral pneumonitis.
We saw a lot of superadded bacterial infections in COVID. You don’t classically see straight forward consolidation with simple viral pneumonitis.
Dynamic air bronchograms appear as basal consolidation worsens.
A great example here where white echogenic fluid can be seen moving up and down the distal small airways with ventilation.
A great example here where white echogenic fluid can be seen moving up and down the distal small airways with ventilation.
And some more dynamic air bronchograms. This is Vs those we would describe as static air bronchograms on CXR.
A final air bronchogram series.
Here, the consolidated, poorly aerated lung takes on the sonographic appearance of the liver! This is known as hepatisation! Bad news!
Here, the consolidated, poorly aerated lung takes on the sonographic appearance of the liver! This is known as hepatisation! Bad news!
We all love to hate finding pleural effusions. A good basal scan can demonstrate black, hypo echoic fluid readily. Here, the lung is squished by pleural fluid and floats around, sometimes like a 🧙♀️ hat! Often, CXR doesn’t pick this up but US smacks you in the face with it!
Another massive effusion with a section of tethered lung. This may be chronic, as inflammation has led to fibrosis and tethering to the diaphragm. Drain fluid IF the patient is compromised or for diagnostics. So it under US guidance🤛👍
Here is a highly proteinaceous exudative effusion in a cancer patient. You see the echogenic fluid swirling about.
A nastily loculated, large pleural effusion. I would run for the hills Vs putting a drain into this mess!
Put it all together in @DanielLICHTENS1’S BLUE protocol to see how amazingly useful Lung #POCUS is!
Happy scanning. All this and more to come in a book chapter with @LukeFlower1 and some fab stuff with @GEHealthcare soon!
Happy scanning. All this and more to come in a book chapter with @LukeFlower1 and some fab stuff with @GEHealthcare soon!
Tagging @zedunow @NephroP @avkwong @amit_pawa @bhca @NixLimerick @aroradrn @cianmcdermott @FTeranMD @cardiacACCP @UltrasoundMD @load_dependent @MJGriksaitis @POCUSClub @ThinkingCC @RubbleEM @rosie_hogg @r_wiersema @iceman_ex @sonophysio @Pocus101 @IMPOCUSFocus @POCUSAcademy
• • •
Missing some Tweet in this thread? You can try to
force a refresh