1/U
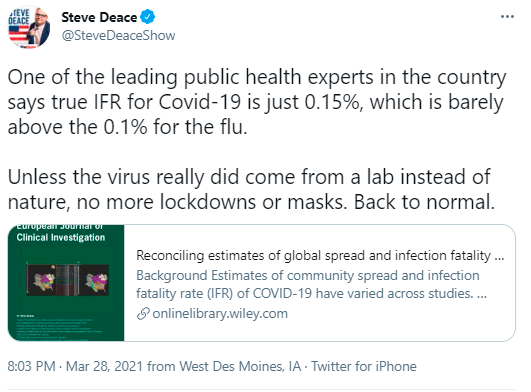
You may recently have heard that COVID-19 has a fatality rate of ~0.15%, making it akin to a bad flu.
In reality, a more accurate fatality rate would be closer to ~0.6%, as per the WHO.
That's ≥10X worse than seasonal flu, and ~100X worse than the 2009 swine flu pandemic.
You may recently have heard that COVID-19 has a fatality rate of ~0.15%, making it akin to a bad flu.
In reality, a more accurate fatality rate would be closer to ~0.6%, as per the WHO.
That's ≥10X worse than seasonal flu, and ~100X worse than the 2009 swine flu pandemic.
2/U
Background:
Infection fatality rate (IFR) is the proportion of people infected with the virus SARS-CoV-2 who die of the disease COVID-19.
IFR for seasonal flu is <0.1%, as per the WHO, among others:
who.int/emergencies/di…
institutefordiseasemodeling.github.io/nCoV-public/an…
Background:
Infection fatality rate (IFR) is the proportion of people infected with the virus SARS-CoV-2 who die of the disease COVID-19.
IFR for seasonal flu is <0.1%, as per the WHO, among others:
who.int/emergencies/di…
https://twitter.com/BallouxFrancois/status/1287198109517451264
institutefordiseasemodeling.github.io/nCoV-public/an…

3/U
So, following @BallouxFrancois, who in their right mind would claim COVID-19 has an IFR comparable with that of seasonal flu?
Well, I can think of at least 2 people.
You likely know who one of them is. 😉
from 2:27 :
So, following @BallouxFrancois, who in their right mind would claim COVID-19 has an IFR comparable with that of seasonal flu?
Well, I can think of at least 2 people.
You likely know who one of them is. 😉
from 2:27 :
4/U
Make that 3 people
"Ioannidis [said it] has an “infection fatality rate that is in the same ballpark as seasonal influenza.”"
buzzfeednews.com/article/stepha…
Gøtzsche:
"[IFR] seems to be about the same as for influenza"
bmj.com/content/371/bm…
Tegnell:
unherd.com/2020/07/sweden…
Make that 3 people
"Ioannidis [said it] has an “infection fatality rate that is in the same ballpark as seasonal influenza.”"
buzzfeednews.com/article/stepha…
Gøtzsche:
"[IFR] seems to be about the same as for influenza"
bmj.com/content/371/bm…
Tegnell:
unherd.com/2020/07/sweden…

5/U
Oh wait, there were at least dozens; see the thread below.
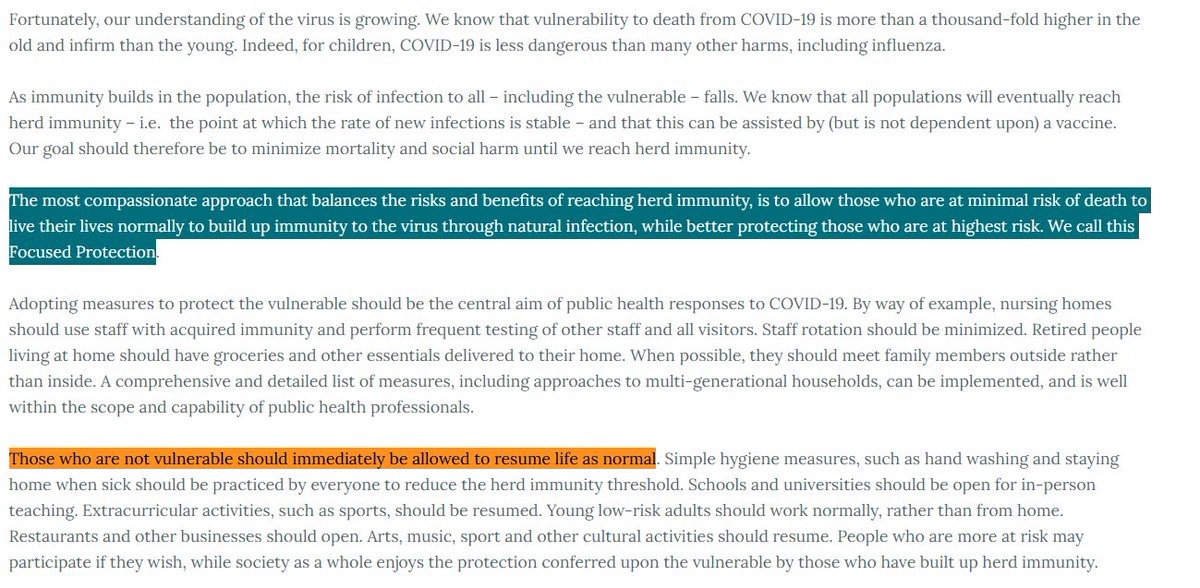
The list includes *all* the authors of the Great Barrington Declaration, the organization behind it, and a lot of people from Stanford.
Probably a coincidence.🤔
archive.is/QLmJt#selectio…
Oh wait, there were at least dozens; see the thread below.
The list includes *all* the authors of the Great Barrington Declaration, the organization behind it, and a lot of people from Stanford.
Probably a coincidence.🤔
https://twitter.com/AtomsksSanakan/status/1319451862123356160
archive.is/QLmJt#selectio…

6/U
The "0.15%" IFR figure seemingly first appeared in an October 2020 paper from Ioannidis.
There he lists at least 2 methods for getting that figure.
As we'll see, there are at least 3 methods overall. And none of them work.
onlinelibrary.wiley.com/doi/pdf/10.111…
The "0.15%" IFR figure seemingly first appeared in an October 2020 paper from Ioannidis.
There he lists at least 2 methods for getting that figure.
As we'll see, there are at least 3 methods overall. And none of them work.
https://twitter.com/AtomsksSanakan/status/1314398873058713601
onlinelibrary.wiley.com/doi/pdf/10.111…

7/U
Method #1:
Cite the World Health Organization (WHO) as saying 10% of people were infected.
Problem with that is WHO officials said *less* than 10% of the population was infected. That includes a WHO expert on this subject.
web.archive.org/web/2020111415…
Method #1:
Cite the World Health Organization (WHO) as saying 10% of people were infected.
Problem with that is WHO officials said *less* than 10% of the population was infected. That includes a WHO expert on this subject.
https://twitter.com/zorinaq/status/1314160525706588168
web.archive.org/web/2020111415…

8/U
Also, from February through October 2020, WHO officials kept saying SARS-CoV-2 had a higher IFR than seasonal influenza.
"Mortality for COVID-19 appears higher than for influenza"
who.int/emergencies/di…
October 12:
who.int/publications/m…
Also, from February through October 2020, WHO officials kept saying SARS-CoV-2 had a higher IFR than seasonal influenza.
"Mortality for COVID-19 appears higher than for influenza"
who.int/emergencies/di…
https://twitter.com/AtomsksSanakan/status/1290693682602156046
October 12:
who.int/publications/m…

9/U
And the WHO continues citing papers that show a higher IFR than Ioannidis claims; that's an IFR much higher than that of seasonal influenza.
They're not even citing his IFR work. That continues into 2021.
January 8, 2021:
apps.who.int/iris/handle/10…
And the WHO continues citing papers that show a higher IFR than Ioannidis claims; that's an IFR much higher than that of seasonal influenza.
They're not even citing his IFR work. That continues into 2021.
https://twitter.com/AtomsksSanakan/status/1374616040664145921
January 8, 2021:
apps.who.int/iris/handle/10…

10/U
So method #1 dies.
Ioannidis moves to a March 2021 paper, i.e. method #2. He conveniently removes mention of the WHO (probably because they contradict him).
That paper under-estimated IFR by using non-representative sampling, among other issues:
So method #1 dies.
Ioannidis moves to a March 2021 paper, i.e. method #2. He conveniently removes mention of the WHO (probably because they contradict him).
That paper under-estimated IFR by using non-representative sampling, among other issues:
https://twitter.com/AtomsksSanakan/status/1375935382139834373
11/U
That leaves method #3, which Ioannidis tried in his October 2021 paper:
Decrease IFR from another one of Ioannidis' IFR studies, by claiming that study focused on places with abnormally large IFR.
That method doesn't work:
onlinelibrary.wiley.com/doi/pdf/10.111…
That leaves method #3, which Ioannidis tried in his October 2021 paper:
Decrease IFR from another one of Ioannidis' IFR studies, by claiming that study focused on places with abnormally large IFR.
That method doesn't work:
https://twitter.com/AtomsksSanakan/status/1375940702761316354
onlinelibrary.wiley.com/doi/pdf/10.111…

11/U
Unsurprisingly, the study Ioannidis adjusts under-estimated IFR by using non-representative samples that over-estimated the number of infections:
But @sschinke also points out under-estimating IFR by under-estimating deaths:
Unsurprisingly, the study Ioannidis adjusts under-estimated IFR by using non-representative samples that over-estimated the number of infections:
https://twitter.com/AtomsksSanakan/status/1341183815176364038
But @sschinke also points out under-estimating IFR by under-estimating deaths:
https://twitter.com/sschinke/status/1376434123468800003

12/U
For example, Ioannidis gives an IFR of 0.06% for Scotland, which is impossible since >0.13% of their total population died of COVID-19.
But he gets that using 47 deaths by April 1, which is too low by at least a factor of 4
web.archive.org/web/2020111809…
For example, Ioannidis gives an IFR of 0.06% for Scotland, which is impossible since >0.13% of their total population died of COVID-19.
But he gets that using 47 deaths by April 1, which is too low by at least a factor of 4
https://twitter.com/AtomsksSanakan/status/1378168166229102593
web.archive.org/web/2020111809…

13/U
Now this might not be Ioannidis' fault, since the death information could have been updated after he checked. He notes such changes in another paper.
But other times the error lies with him.
academic.oup.com/ije/advance-ar…
Now this might not be Ioannidis' fault, since the death information could have been updated after he checked. He notes such changes in another paper.
But other times the error lies with him.
https://twitter.com/AtomsksSanakan/status/1343680974383681536
https://twitter.com/AtomsksSanakan/status/1341314669928177664
academic.oup.com/ije/advance-ar…

14/U
So I tried to address these death issues in the randomized/representative sampling studies that Ioannidis collected + adjusted for method #3.
After I got a median IFR of 0.58% (~0.6%).
A bit higher than before:
So I tried to address these death issues in the randomized/representative sampling studies that Ioannidis collected + adjusted for method #3.
After I got a median IFR of 0.58% (~0.6%).
A bit higher than before:
https://twitter.com/AtomsksSanakan/status/1341322079526895616
https://twitter.com/AtomsksSanakan/status/1341334316673019905
15/U
But that ~0.6% IFR matches what WHO officials said for months before *and after* they were aware of Ioannidis' work (see part 8/U), including his work that was submitted to the Bulletin of the WHO.
That fits with the following hypothesis.
But that ~0.6% IFR matches what WHO officials said for months before *and after* they were aware of Ioannidis' work (see part 8/U), including his work that was submitted to the Bulletin of the WHO.
That fits with the following hypothesis.
https://twitter.com/AtomsksSanakan/status/1378488848288784391

16/U
WHO experts (😉) knew how to recognize representative sampling. So they removed studies with non-representative sampling from Ioannidis' analysis + addressed his errors on deaths.
That led to their 0.6% IFR
And they said not to cite his flawed work
apps.who.int/iris/bitstream…
WHO experts (😉) knew how to recognize representative sampling. So they removed studies with non-representative sampling from Ioannidis' analysis + addressed his errors on deaths.
That led to their 0.6% IFR
And they said not to cite his flawed work
apps.who.int/iris/bitstream…

17/U
That was just a hypothesis/conjecture. But it does neatly explain the WHO's IFR + their response to Ioannidis' work.
In any event, the '0.15% IFR' claim is nonsense.
It's likely closer to ~0.6%; much worse than seasonal flu
sciencedirect.com/science/articl…
That was just a hypothesis/conjecture. But it does neatly explain the WHO's IFR + their response to Ioannidis' work.
In any event, the '0.15% IFR' claim is nonsense.
It's likely closer to ~0.6%; much worse than seasonal flu
https://twitter.com/AtomsksSanakan/status/1323074012122124288
sciencedirect.com/science/articl…

18/U
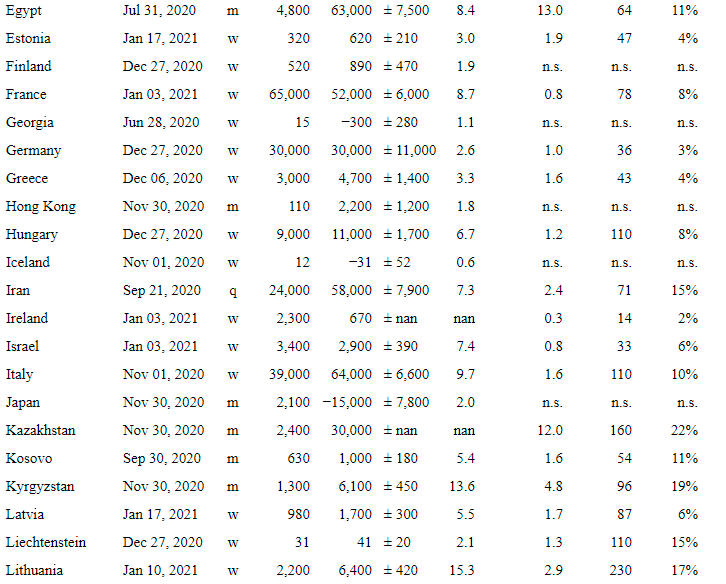
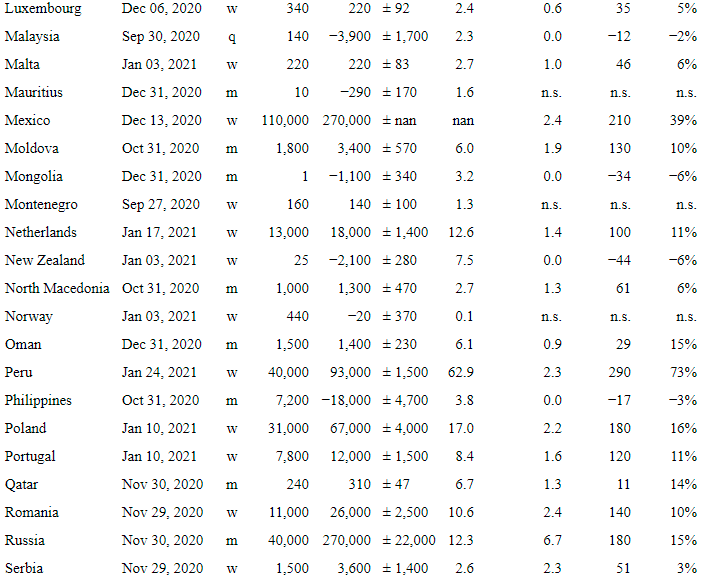
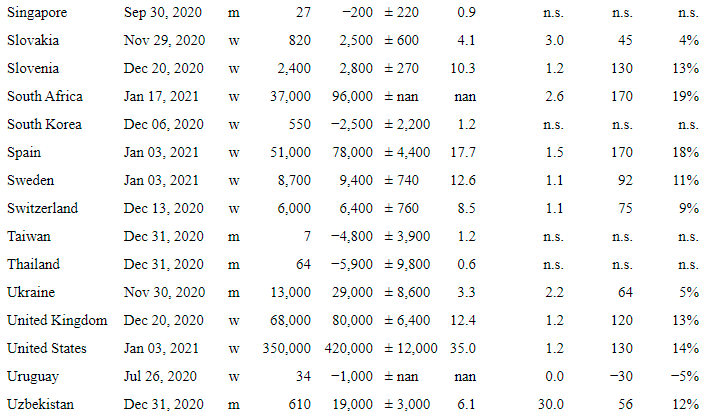
Some people may want to check the median IFR of ~0.6% from part 14/U (I miswrote 0.61% as 0.58%).
So below is a numbered list of studies from Ioannidis' paper, along with which studies I used:
web.archive.org/web/2020111809…
Some people may want to check the median IFR of ~0.6% from part 14/U (I miswrote 0.61% as 0.58%).
So below is a numbered list of studies from Ioannidis' paper, along with which studies I used:
https://twitter.com/AtomsksSanakan/status/1341281002065436673https://pbs.twimg.com/media/Ep0vp0ZWwAAimq2?format=png&name=900x900https://pbs.twimg.com/media/Ep0vp0ZWwAAimq2?format=png&name=900x900
https://twitter.com/AtomsksSanakan/status/1341322079526895616
web.archive.org/web/2020111809…

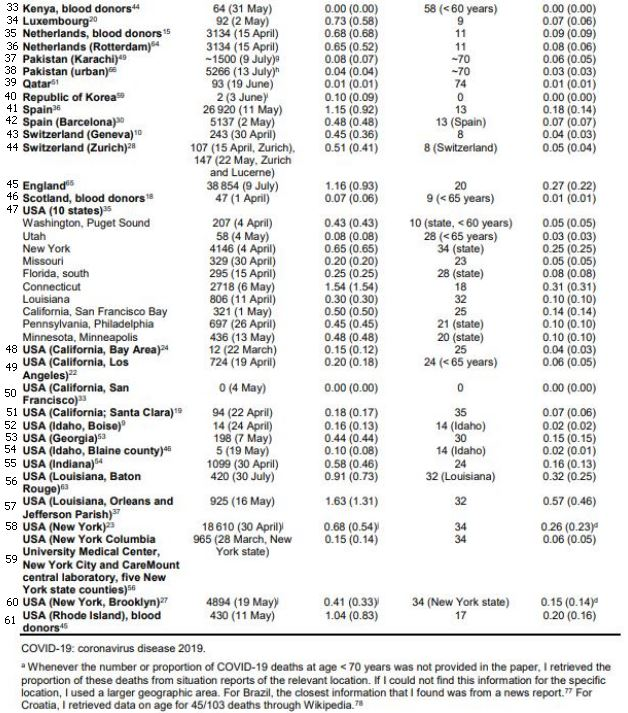
19/U
Study #49 for Los Angeles County should be left out.
Ioannidis' IFR of 0.18% is impossible since >0.22% of the county died of COVID-19. Also had an accelerating outbreak.
dashboard.publichealth.lacounty.gov/covid19_survei…
coronavirus.jhu.edu/us-map
link.springer.com/article/10.100…
Study #49 for Los Angeles County should be left out.
Ioannidis' IFR of 0.18% is impossible since >0.22% of the county died of COVID-19. Also had an accelerating outbreak.
dashboard.publichealth.lacounty.gov/covid19_survei…
coronavirus.jhu.edu/us-map
https://twitter.com/AtomsksSanakan/status/1377280277244997637
link.springer.com/article/10.100…

20/U
~0.6% IFR is consistent with other non-Ioannidis studies.
0.68% (0.53–0.82%)
0.76% (0.37–1.15%) for higher-quality studies
sciencedirect.com/science/articl…
0.79% (0.68–0.92%)
median range: 0.24–1.49%
nature.com/articles/s4158…
imperial.ac.uk/media/imperial…
~0.6% IFR is consistent with other non-Ioannidis studies.
https://twitter.com/AtomsksSanakan/status/1336442679689965570
0.68% (0.53–0.82%)
0.76% (0.37–1.15%) for higher-quality studies
sciencedirect.com/science/articl…
0.79% (0.68–0.92%)
median range: 0.24–1.49%
nature.com/articles/s4158…
imperial.ac.uk/media/imperial…

21/U
Part 5/U included the wrong link be mistake. The thread it's referring to is below
Part 5/U included the wrong link be mistake. The thread it's referring to is below
https://twitter.com/AtomsksSanakan/status/1358014925021581314

22/U
Thread with more details on the Scotland deaths mentioned in parts 11/U and 13/U:
Thread with more details on the Scotland deaths mentioned in parts 11/U and 13/U:
https://twitter.com/sschinke/status/1378540317989687298
23/U
IFR increases with age
link.springer.com/article/10.100…
cdc.gov/coronavirus/20…
medrxiv.org/content/10.110…
So we can check if countries with ages close to the global median have IFRs near Ioannidis' global 0.15%
web.archive.org/web/2021040513…
IFR increases with age
link.springer.com/article/10.100…
cdc.gov/coronavirus/20…
medrxiv.org/content/10.110…
https://twitter.com/AtomsksSanakan/status/1363580232339517444
So we can check if countries with ages close to the global median have IFRs near Ioannidis' global 0.15%
https://twitter.com/gianlucac1/status/1378999875996680194
web.archive.org/web/2021040513…

24/U
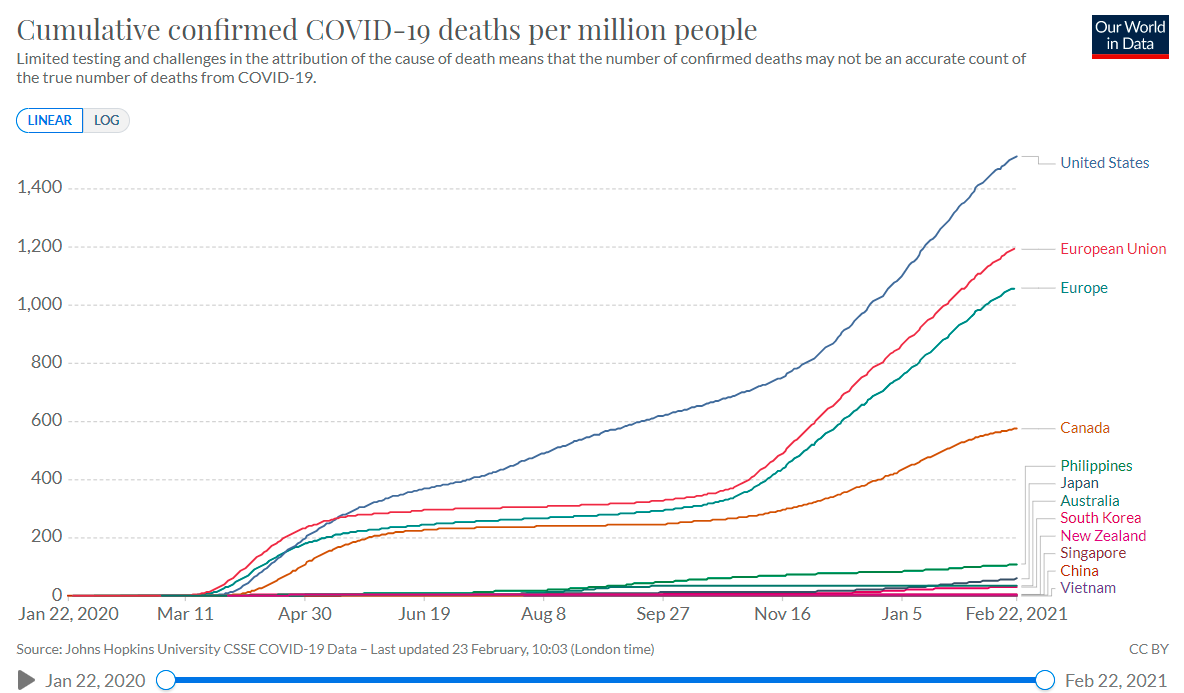
On how well countries catch COVID-19 deaths:
medrxiv.org/content/10.110…
github.com/akarlinsky/wor…
Colombia's death reporting is pretty good, with an IFR of ~0.4% or more.
blogs.worldbank.org/developmenttal…
On how well countries catch COVID-19 deaths:
medrxiv.org/content/10.110…
github.com/akarlinsky/wor…
https://twitter.com/hippopedoid/status/1377605778731896832
Colombia's death reporting is pretty good, with an IFR of ~0.4% or more.
https://twitter.com/AtomsksSanakan/status/1371858714240675842
https://twitter.com/gdemom/status/1371603103515049985
blogs.worldbank.org/developmenttal…

25/U
Peru under-estimates COVID-19 deaths, so its IFR should be >>0.5%.
seroprevalence:
dge.gob.pe/portal/docs/to…
web.archive.org/web/2020122009…
thelancet.com/journals/eclin…
dge.gob.pe/portalnuevo/wp…
28 - 35min: facebook.com/minsaperu/vide…
deaths:
covid19.minsa.gob.pe/sala_situacion…
Peru under-estimates COVID-19 deaths, so its IFR should be >>0.5%.
seroprevalence:
dge.gob.pe/portal/docs/to…
web.archive.org/web/2020122009…
thelancet.com/journals/eclin…
dge.gob.pe/portalnuevo/wp…
28 - 35min: facebook.com/minsaperu/vide…
deaths:
covid19.minsa.gob.pe/sala_situacion…
https://twitter.com/hippopedoid/status/1377605778731896832

26/U
Iran under-estimates deaths, so its IFR should be >0.4%
onlinelibrary.wiley.com/doi/full/10.10…
medrxiv.org/content/10.110…
seroprevalence:
- nationwide:
medrxiv.org/content/10.110…
(regions:
thelancet.com/journals/lanin…
wwwnc.cdc.gov/eid/article/27…
deaths:
covid19.who.int/region/emro/co…
Iran under-estimates deaths, so its IFR should be >0.4%
onlinelibrary.wiley.com/doi/full/10.10…
medrxiv.org/content/10.110…
seroprevalence:
- nationwide:
medrxiv.org/content/10.110…
(regions:
thelancet.com/journals/lanin…
wwwnc.cdc.gov/eid/article/27…
https://twitter.com/AtomsksSanakan/status/1332826132341788673)
deaths:
covid19.who.int/region/emro/co…
27/U
Brazil slightly under-estimates deaths, with an IFR >0.6%.
seroprevalence:
thelancet.com/journals/langl…
ncbi.nlm.nih.gov/pmc/articles/P… (excludes nursing home deaths, lowering IFR)
estado.rs.gov.br/estudo-epidemi…
deaths:
transparencia.registrocivil.org.br/especial-covid
web.archive.org/web/2021040513…
Brazil slightly under-estimates deaths, with an IFR >0.6%.
seroprevalence:
https://twitter.com/AtomsksSanakan/status/1341325914647441408
thelancet.com/journals/langl…
ncbi.nlm.nih.gov/pmc/articles/P… (excludes nursing home deaths, lowering IFR)
estado.rs.gov.br/estudo-epidemi…
deaths:
transparencia.registrocivil.org.br/especial-covid
web.archive.org/web/2021040513…

28/U
So for 4 countries with randomized seroprevalence studies + median ages near the global median:
- IFR is larger than Ioannidis' global 0.15%
- IFR is compatible with the WHO's ~0.6%
Why are people still peddling Ioannidis' shoddy estimate?
🤔
publichealthontario.ca/-/media/docume…
So for 4 countries with randomized seroprevalence studies + median ages near the global median:
- IFR is larger than Ioannidis' global 0.15%
- IFR is compatible with the WHO's ~0.6%
Why are people still peddling Ioannidis' shoddy estimate?
🤔
publichealthontario.ca/-/media/docume…

29/U
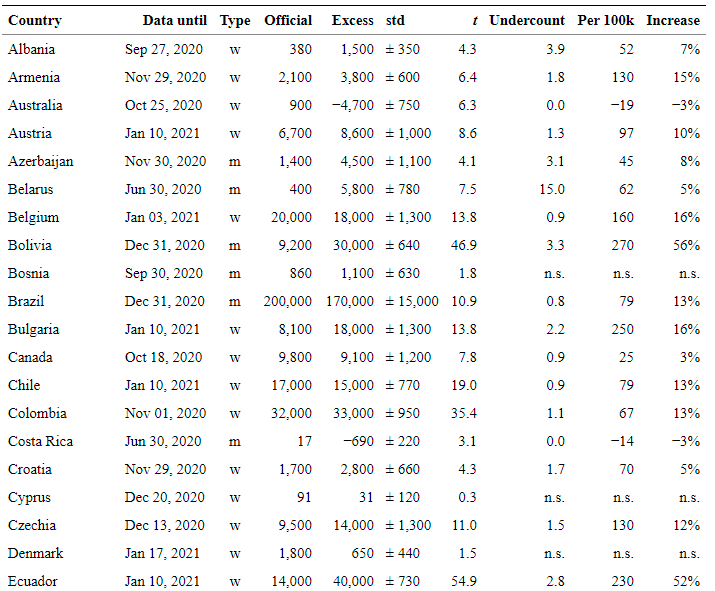
Also, excess deaths in 24/U + 25/U are a good indicator of under-estimated COVID-19 deaths, regardless of Ioannidis' falsehoods on that.
Other indicators also point to under-estimated COVID-19 deaths.
Also, excess deaths in 24/U + 25/U are a good indicator of under-estimated COVID-19 deaths, regardless of Ioannidis' falsehoods on that.
Other indicators also point to under-estimated COVID-19 deaths.
https://twitter.com/AtomsksSanakan/status/1354483530307395586
https://twitter.com/AtomsksSanakan/status/1376012415830200324
• • •
Missing some Tweet in this thread? You can try to
force a refresh