
Wonderful opportunity to hear the great and the good discussing evidence underlying SARS-CoV-2 transmission & optimal mitigation: the most immediately pressing topics for humanity.
@kprather88 @DFisman and Prof John Conly
#COVIDisAirborne
/1
@kprather88 @DFisman and Prof John Conly
#COVIDisAirborne
/1


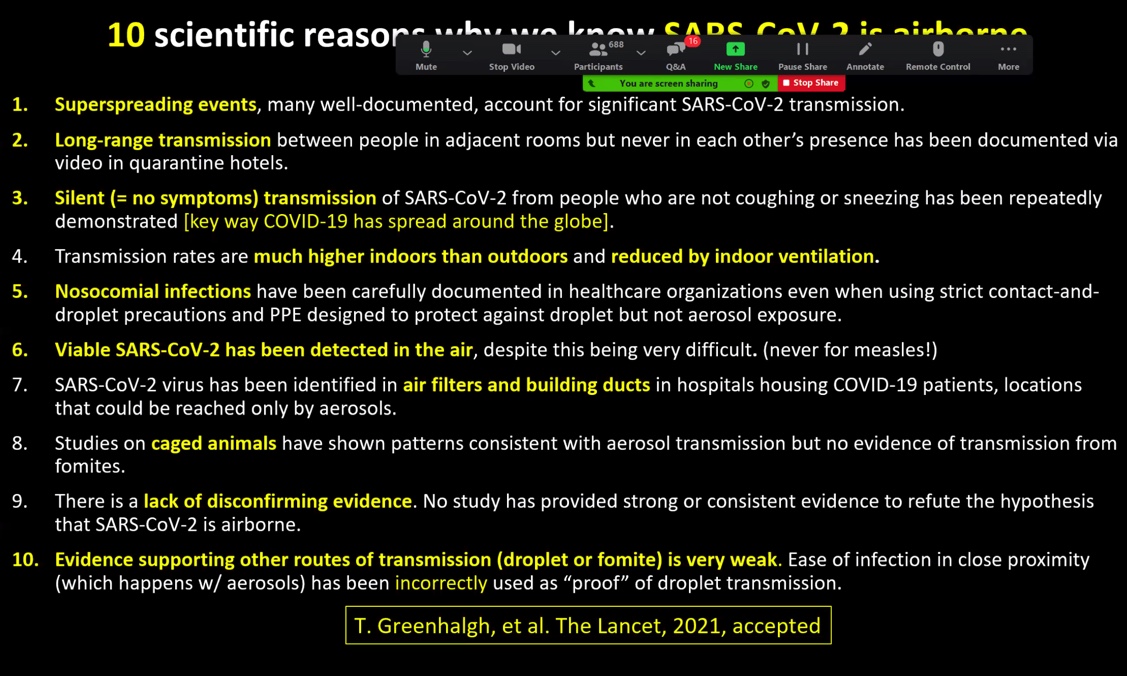
@kprather88 summary:
Short and long-range inhalation of aerosols is the dominant route for transmission, with extensive & rigorous supportive data.
'Droplets don't shoot out and turn around back' - chorister event
'Droplets don't do bends' - ferret model proving airborne route
Short and long-range inhalation of aerosols is the dominant route for transmission, with extensive & rigorous supportive data.
'Droplets don't shoot out and turn around back' - chorister event
'Droplets don't do bends' - ferret model proving airborne route

@kprather88 more:
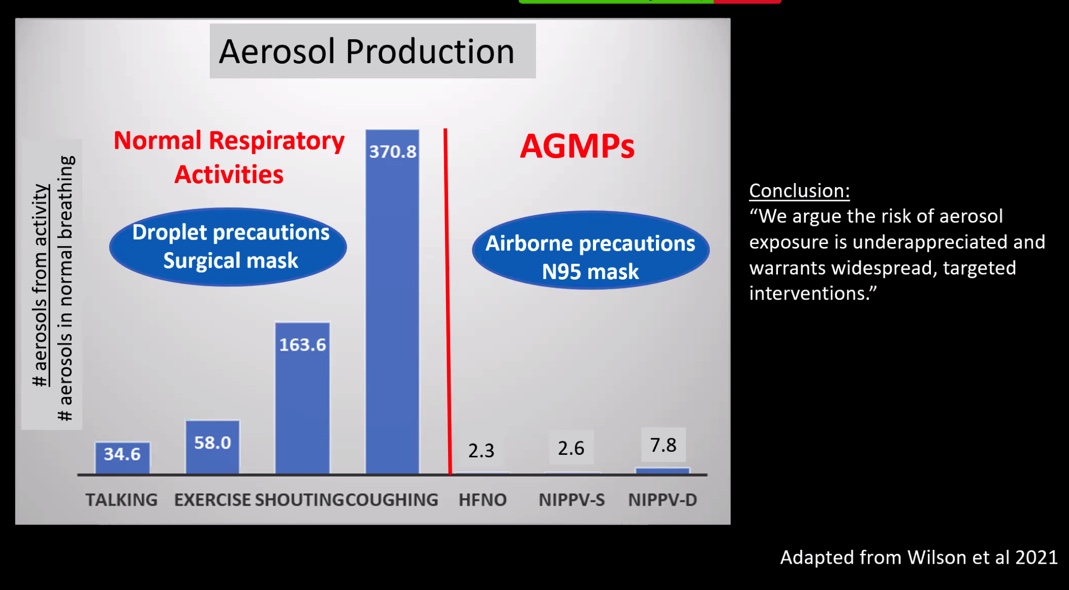
Humans are aerosol generating people!
AGMPs release fewer aerosols [for transmission], yet WHO guidelines suggest HCWs only require N95 masks for AGMPs.
[ed: this dogma needs to die - it's responsible for the infection &/or death of 1000's of HCWs globally]
Humans are aerosol generating people!
AGMPs release fewer aerosols [for transmission], yet WHO guidelines suggest HCWs only require N95 masks for AGMPs.
[ed: this dogma needs to die - it's responsible for the infection &/or death of 1000's of HCWs globally]
@kprather88 more:
WHO SARS-CoV-2 IPC Scientific Briefing July 2020 needs an urgent update in light of every aspect of [alleged] gaps in research being addressed.
[ed: our lives are on the line here 🙏]
#COVIDisAirborne @trishgreenhalgh @microlabdoc @mjb302 @Linzofm87
WHO SARS-CoV-2 IPC Scientific Briefing July 2020 needs an urgent update in light of every aspect of [alleged] gaps in research being addressed.
[ed: our lives are on the line here 🙏]
#COVIDisAirborne @trishgreenhalgh @microlabdoc @mjb302 @Linzofm87

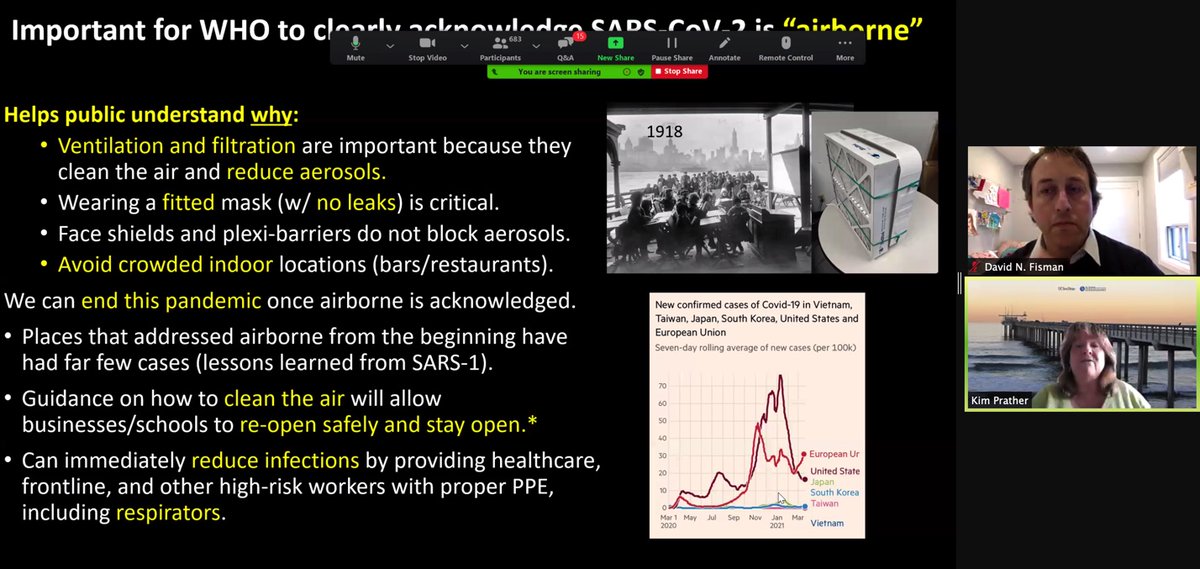
@kprather88: why it is important for @WHO to clearly acknowledge that SARS-CoV-2 is 'airborne'
@mvankerkhove @NjbBari3
@mvankerkhove @NjbBari3
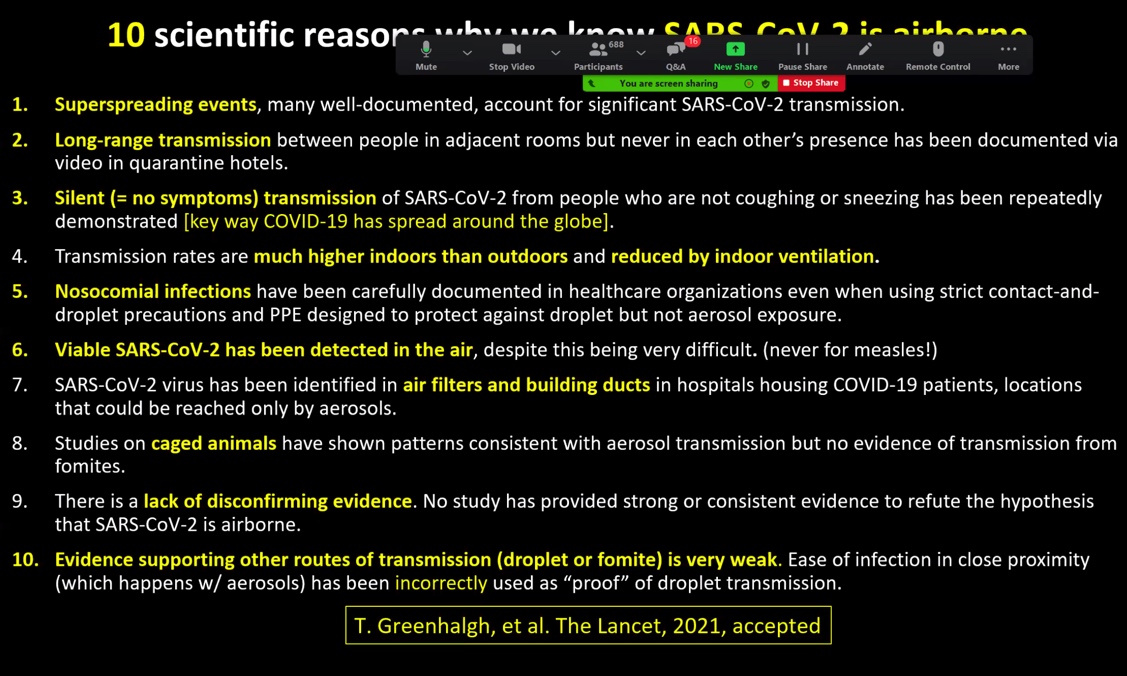
@kprather88 if anyone still needs convincing:
@LABailey @thedalstonyears @ShaunLintern @richardhorton1 @JeremyFarrar @PeterHorby @ProfCalumSemple @CMO_England @uksciencechief @AnthonyMangnal1 @GregClarkMP @MattHancock @theRCN
#COVIDisAirborne
@LABailey @thedalstonyears @ShaunLintern @richardhorton1 @JeremyFarrar @PeterHorby @ProfCalumSemple @CMO_England @uksciencechief @AnthonyMangnal1 @GregClarkMP @MattHancock @theRCN
#COVIDisAirborne
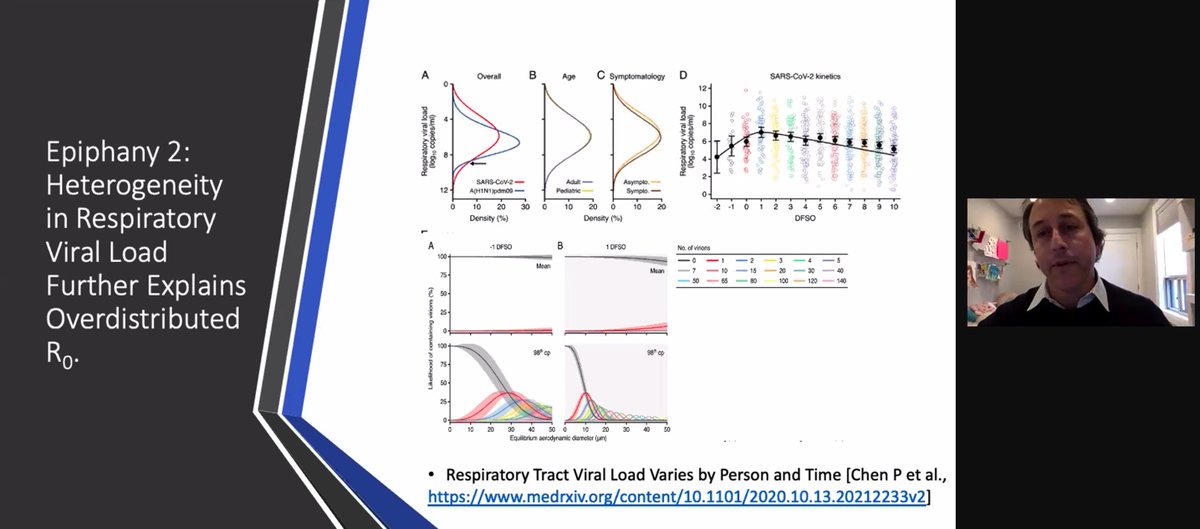
@DFisman only had 5 minutes but shared his 'epiphanies'
'It's time to let the science speak'
'It's time to treat [SARS-CoV-2] as predominant airborne spread'
#COVIDisAirborne
'It's time to let the science speak'
'It's time to treat [SARS-CoV-2] as predominant airborne spread'
#COVIDisAirborne

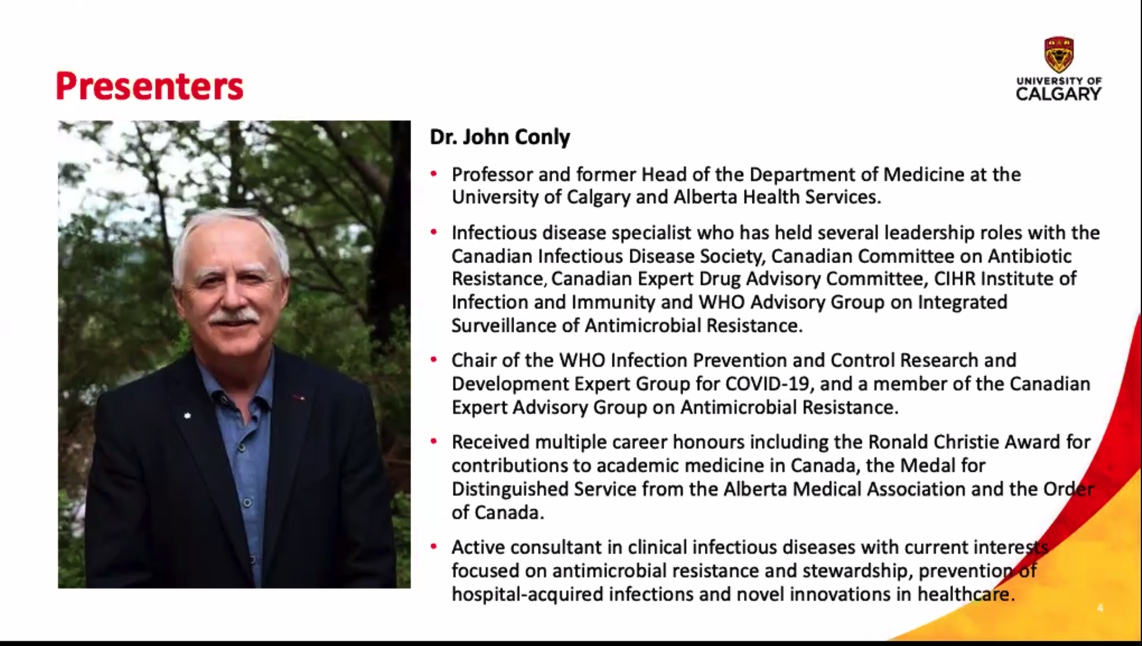
Prof John Conly. In case you've forgotten: he's a VIP with respect to global health policy.
So we'd better hope he's up to speed on the latest science & isn't trying to hold on to respiratory virus transmission concepts based on dogma, bad science and/or bias, right?
So we'd better hope he's up to speed on the latest science & isn't trying to hold on to respiratory virus transmission concepts based on dogma, bad science and/or bias, right?
Confession: for me, his presentation started very badly as it was exactly the same opening slides & discussion as in his July 2020 talk.
Best summarised as a masterclass in medical misinformation.
Check out the thread and you'll see why.
Best summarised as a masterclass in medical misinformation.
Check out the thread and you'll see why.
https://twitter.com/DRTomlinsonEP/status/1380272045339082755?s=20
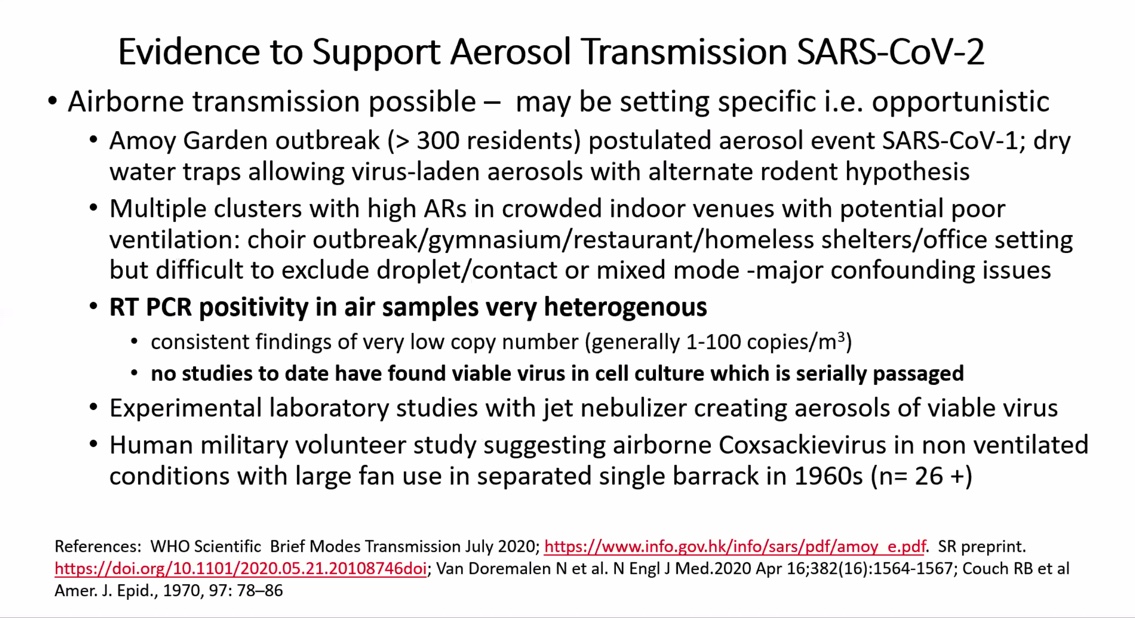
Summary: Does anyone else think these two slides alone provide evidence indicating that Prof Conly is importantly biased against airborne transmission of SARS-CoV-2? He's omitted a vast body of data supporting airborne.
Does anyone have any idea what his true motivations are?
Does anyone have any idea what his true motivations are?

Amazingly, Prof John Conly admitted that airborne transmission of SARS-CoV-2 can occur, but that "it's situational".
I seem to recall similar statements from @angie_rasmussen and/or @SaskiaPopescu on this platform in recent weeks.
Is this a clear enough public health message?
I seem to recall similar statements from @angie_rasmussen and/or @SaskiaPopescu on this platform in recent weeks.
Is this a clear enough public health message?
More:
Face touching getting a mention here: maybe SARS-CoV-2 neuronal infection creates disinhibition of face touching behaviour?
It's possible I guess. But direct aerosol-bound viral binding of alveolar type II pneumocyte ACE2 receptors with TMPRSS2 is so much easier, right?
Face touching getting a mention here: maybe SARS-CoV-2 neuronal infection creates disinhibition of face touching behaviour?
It's possible I guess. But direct aerosol-bound viral binding of alveolar type II pneumocyte ACE2 receptors with TMPRSS2 is so much easier, right?

Last slide: nice attempt to suggest the airborne transmission 'world of science' [my words] is lacking rigour.
This tactic is a great ploy for politicians campaigning or aggressive advertising against competitor brands but has absolutely NO ROLE in scientific discourse.
This tactic is a great ploy for politicians campaigning or aggressive advertising against competitor brands but has absolutely NO ROLE in scientific discourse.

Notable absences from Prof Conly's talk:
No attempt to explain how superspreading occurs with his 'transmission model' limiting airborne spread to 'situational'.
Nothing to counter the animal models which prove airborne transmission.
No apology to HCWs for @WHO PPE policy.
No attempt to explain how superspreading occurs with his 'transmission model' limiting airborne spread to 'situational'.
Nothing to counter the animal models which prove airborne transmission.
No apology to HCWs for @WHO PPE policy.

Closing Qs: 10 mins.
JC: accepted airborne transmission can occur but that it is 'situational'.
JC: regarding aerosol transmission, 'I would like to see much higher levels of scientific evidence including some basic science.'
MUCH higher: what's his definition of 'much'?
JC: accepted airborne transmission can occur but that it is 'situational'.
JC: regarding aerosol transmission, 'I would like to see much higher levels of scientific evidence including some basic science.'
MUCH higher: what's his definition of 'much'?
Fantastic exchange on the Q of why in early 2020, WHO did not use the precautionary principle & treat SARS-CoV-2 as an airborne transmitted virus.
@DFisman 'It's time to treat as predominant airborne spread'
Conly: 'I couldn't disagree more'
Reasons given? Next tweet...
@DFisman 'It's time to treat as predominant airborne spread'
Conly: 'I couldn't disagree more'
Reasons given? Next tweet...

Conly: 'you need to consider the harms of N95 masks'
- Acne
- Eczema
- Conjunctivitis
- CO2 retention
- Low O2 saturations in pregnant women
In this order. Honest.
Q for HCWs: given the choice, would you risk death/long covid/onward transmissions with FRSM, or 🖕 with N95?
- Acne
- Eczema
- Conjunctivitis
- CO2 retention
- Low O2 saturations in pregnant women
In this order. Honest.
Q for HCWs: given the choice, would you risk death/long covid/onward transmissions with FRSM, or 🖕 with N95?
So there you have it.
In a nutshell:
@kprather88 'Once we acknowledge it is airborne we can fix it.'
@DFisman 'It's time to treat as predominant airborne spread.'
Prof John Conly 'Airborne transmission can occur: it's situational.'
#COVIDisAirborne @lisa_iannattone
END
In a nutshell:
@kprather88 'Once we acknowledge it is airborne we can fix it.'
@DFisman 'It's time to treat as predominant airborne spread.'
Prof John Conly 'Airborne transmission can occur: it's situational.'
#COVIDisAirborne @lisa_iannattone
END
• • •
Missing some Tweet in this thread? You can try to
force a refresh















