A summary thread of the latest #REACT survey from @imperialcollege on England infectivity.
The headline is very good news, prevalence has halved since the last round, falling from 0.20% to 0.10%, with R at 0.9 between the rounds.
Round 11 is between April 15 and May 3.
1/
The headline is very good news, prevalence has halved since the last round, falling from 0.20% to 0.10%, with R at 0.9 between the rounds.
Round 11 is between April 15 and May 3.
1/

115 positive samples were obtained from 127k tests. Note the slightly lower number of tests this round, which the report notes is due to a lower response rate, suggesting a lower interest in participants as the situation improves.
2/
2/

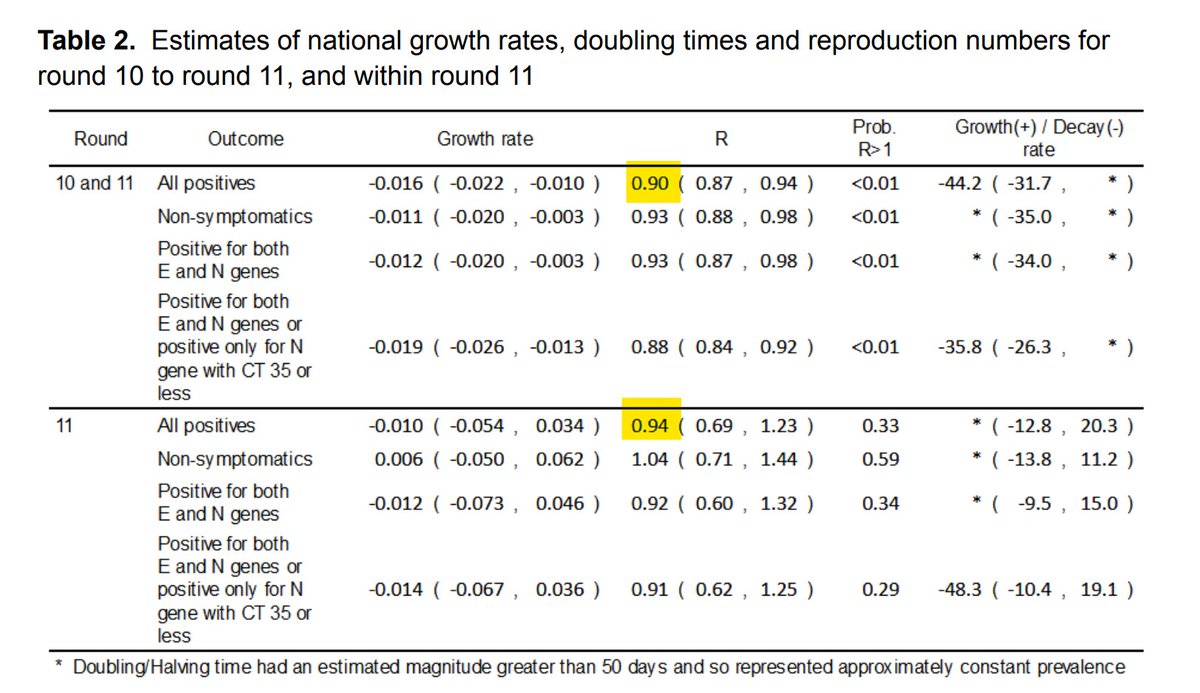
Between rounds, R is put at 0.9, though slightly higher at 0.94 within the round. This is consistent with recent SAGE views, and not unexpected as the lockdown restrictions are gradually eased.
3/
3/
By region, the SE is the only area to show an increase between R10 and R11. Although the CI's are wide, it's considered that there is a very high probability that the underlying situation is of R being greater than 1.
4/
4/


By age, there's a similar situation with the 25-34 age groups of a small overall increase, now at 0.21% double the overall figure.
The biggest fall has been a two thirds fall in the 55-64 group, likely reflective of that group acquiring vaccine protection between the rounds.
5/
The biggest fall has been a two thirds fall in the 55-64 group, likely reflective of that group acquiring vaccine protection between the rounds.
5/

It's great to see the clear disconnect between deaths (in red) and prevalence since mid January, clearly showing that even if infected, the vaccine prevents serious illness and death.
6/
6/

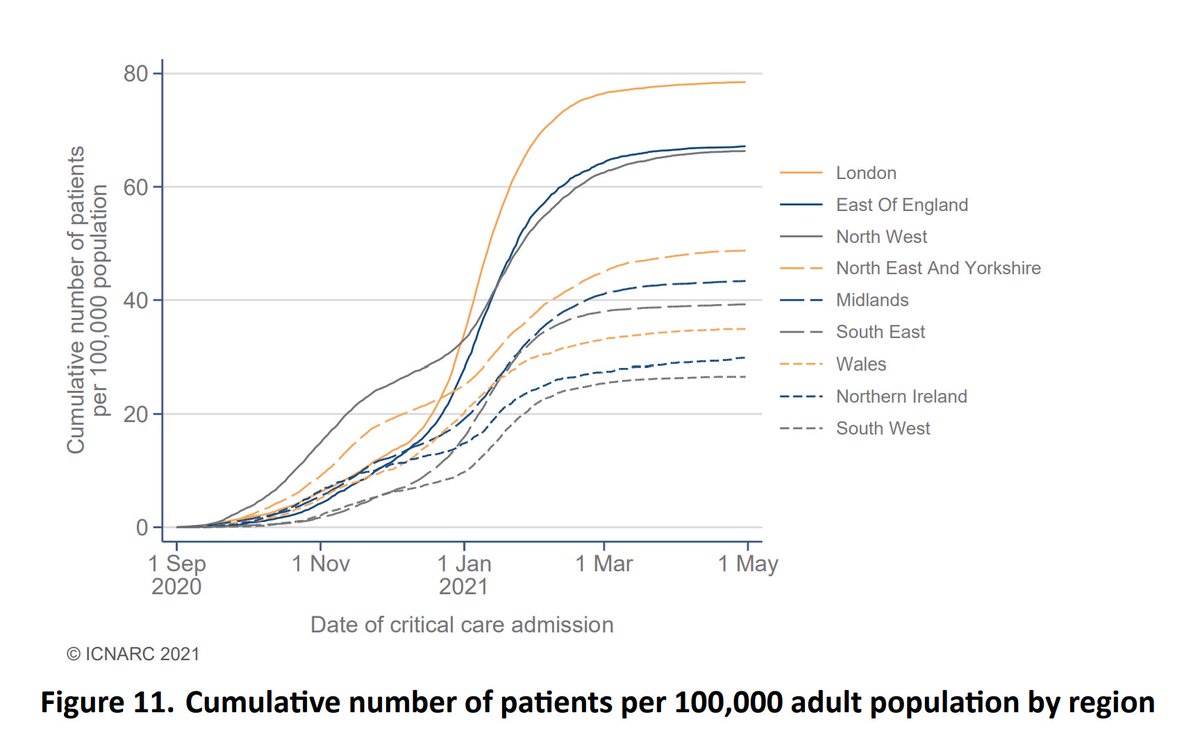
There's an effect on hospitalisations too, but it's much less marked, consistent with predictions made as the roll-out started that deaths would fall faster than hospitalisations.
7/
7/

The report notes the presence of B.1.617.2 in around 7.5% of the cases for which a lineage could be identified, although this is only 2 out of 26 samples. The remainder were B.1.1.7.
8/
8/

Note that REACT is a randomly sampled survey, which is the best way to ensure a true representation of the population, and which isn't affected by factors such as number of available tests.
9/
9/
As one example, the vaccine may be increasing the proportion of cases which are asymptomatic. These are less likely to be picked up by PHE testing, or by surveillance methods reliant on self-reporting.
10/
10/
So it is one of several methods of measuring the level and direction of prevalence, all of which have their benefits and weaknesses, and which should be considered in the whole rather than individually to assess the current position of the pandemic.
spiral.imperial.ac.uk/bitstream/1004…
11/END
spiral.imperial.ac.uk/bitstream/1004…
11/END
• • •
Missing some Tweet in this thread? You can try to
force a refresh