How effective are vaccines vs severe & all disease, death, infection, & transmission?
Very nice collection of studies assessing different aspects of vaccine protection by Julia Shapiro (on twitter?) @nataliexdean @betzhallo @ilongini & 2 others.
Thread
medrxiv.org/content/10.110…
Very nice collection of studies assessing different aspects of vaccine protection by Julia Shapiro (on twitter?) @nataliexdean @betzhallo @ilongini & 2 others.
Thread
medrxiv.org/content/10.110…
Study has data on many different measures of protection:
all infection (symp + asymp), all symptomatic (mild+severe), severe, hospitalization, death, & transmission,
for 8 vaccines: Moderna, Pfizer, Novavax, Astrazeneca, Sinopharm, Sinovac, Sputnik, J&J,
3 variants&
1&2 doses
all infection (symp + asymp), all symptomatic (mild+severe), severe, hospitalization, death, & transmission,
for 8 vaccines: Moderna, Pfizer, Novavax, Astrazeneca, Sinopharm, Sinovac, Sputnik, J&J,
3 variants&
1&2 doses

For those wanting to understand relationships among different vaccine efficacy measures more, recent preprint @mlipsitch @kahnrebecca, lays it out nicely. doi.org/10.1101/2021.0…;
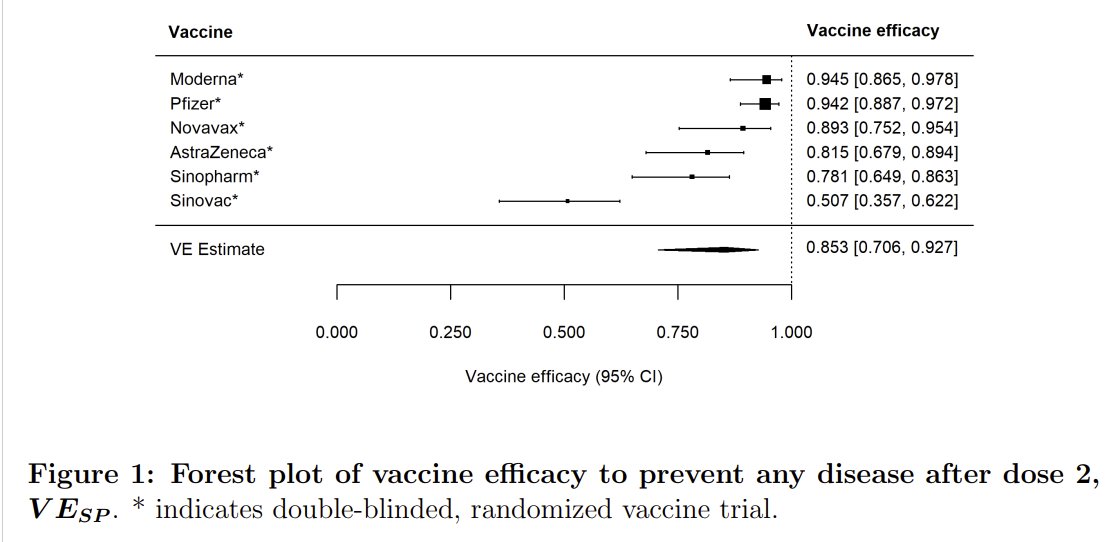
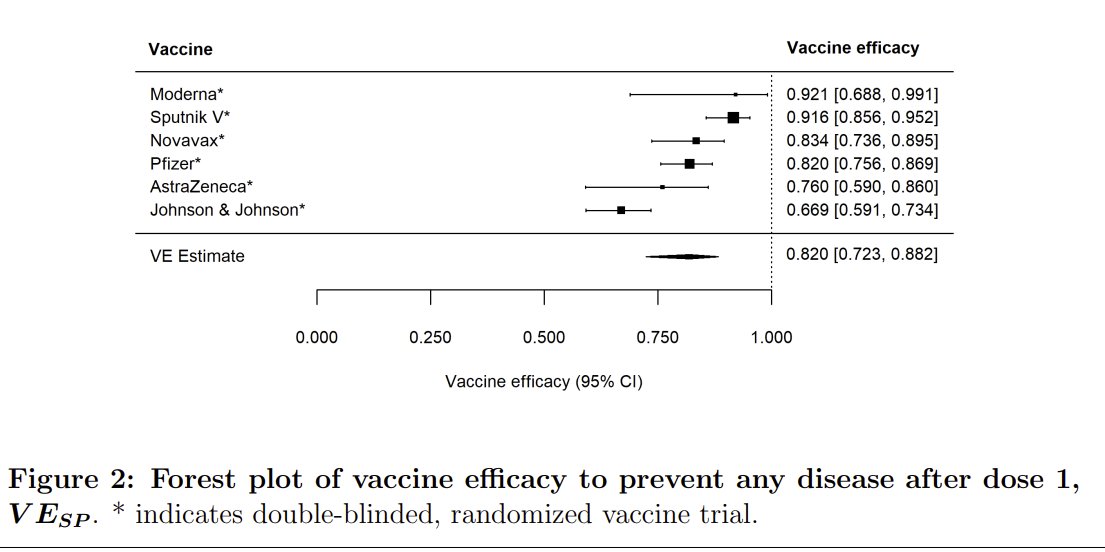
Results are shown in 9 Figures. Here are 1st 4:
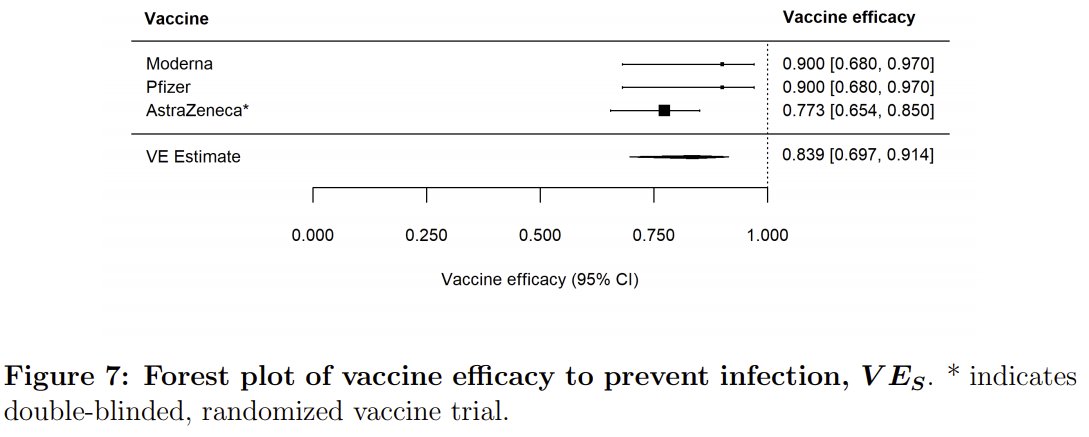
All disease, post-dose 2: 85% (95% CI: 71 - 93%)
dose 1: 82% (95% CI: 72 - 88%)
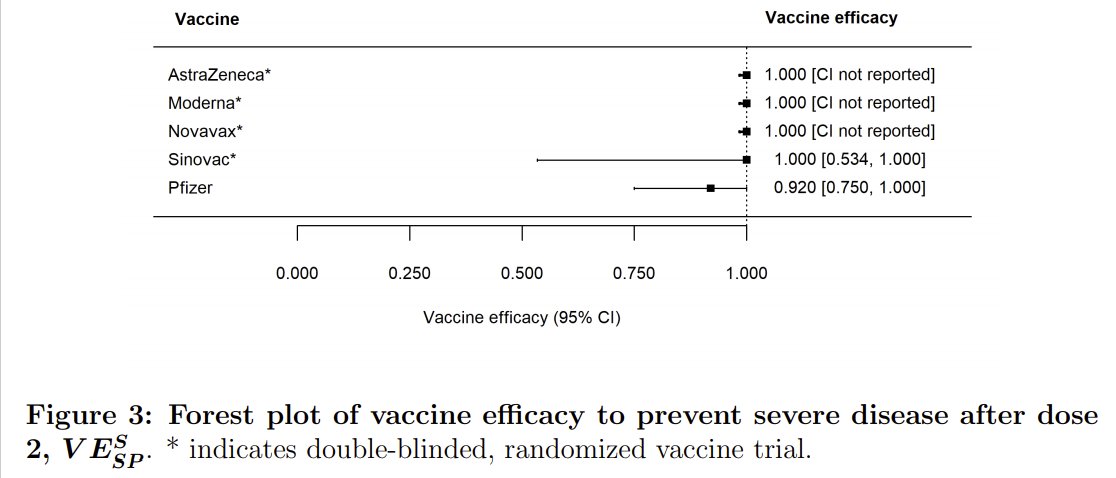
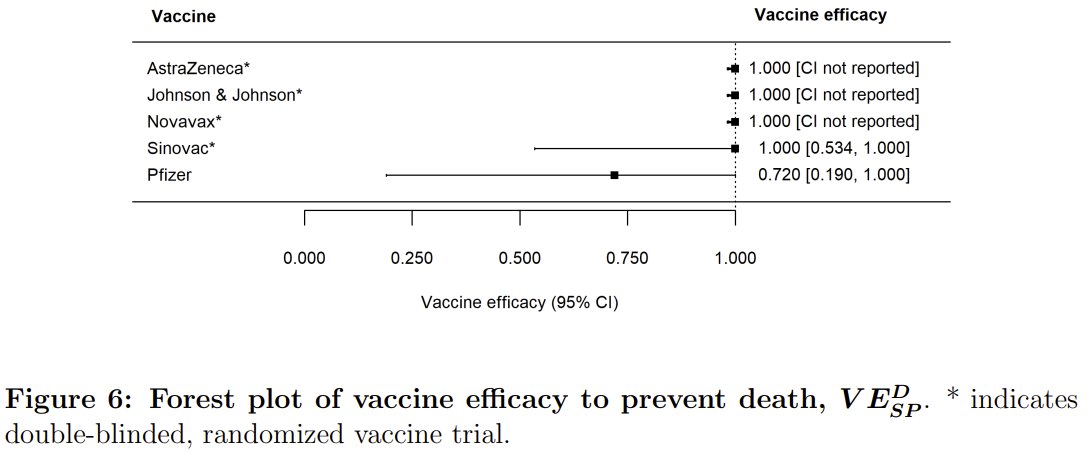
Severe disease post-dose 2: no overall estimate b/c no CI for many vaccines (see below)
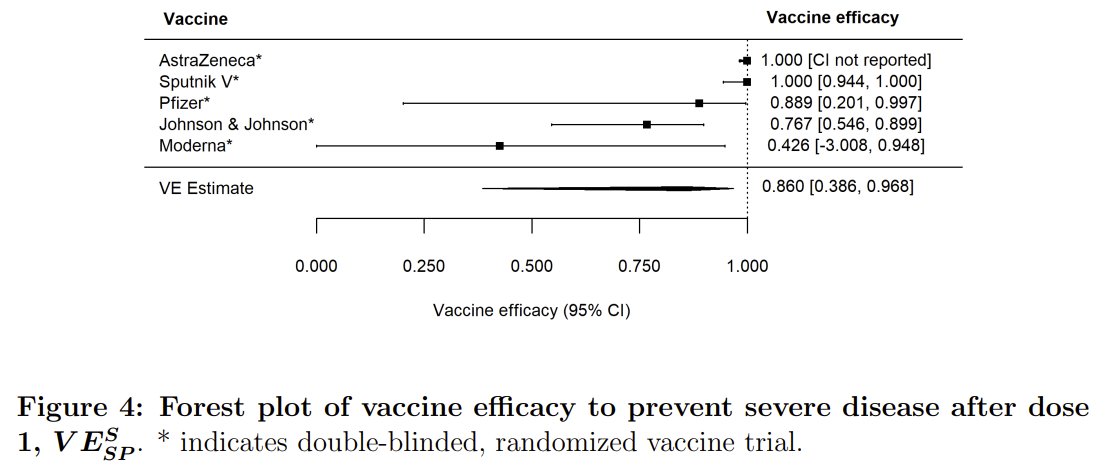
dose 1: 86% (95% CI: 39 - 97%)
See also
All disease, post-dose 2: 85% (95% CI: 71 - 93%)
dose 1: 82% (95% CI: 72 - 88%)
Severe disease post-dose 2: no overall estimate b/c no CI for many vaccines (see below)
dose 1: 86% (95% CI: 39 - 97%)
See also
https://twitter.com/DiseaseEcology/status/1374241297238618112
2nd 4:
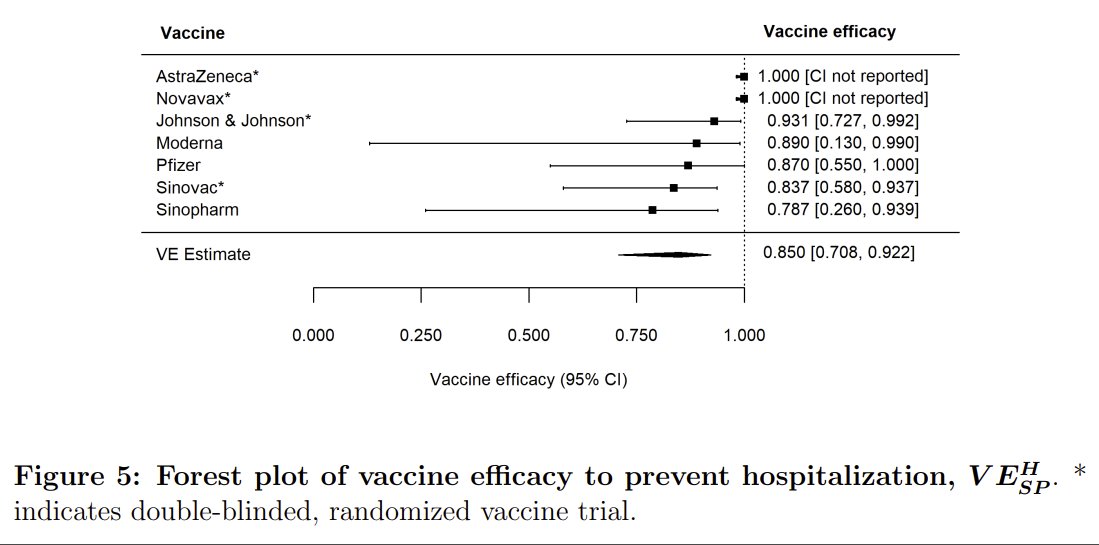
Protection vs
hospitalization 85% (71-92%)
death (no overall estimate)
all infection 83.9% (70-91%)
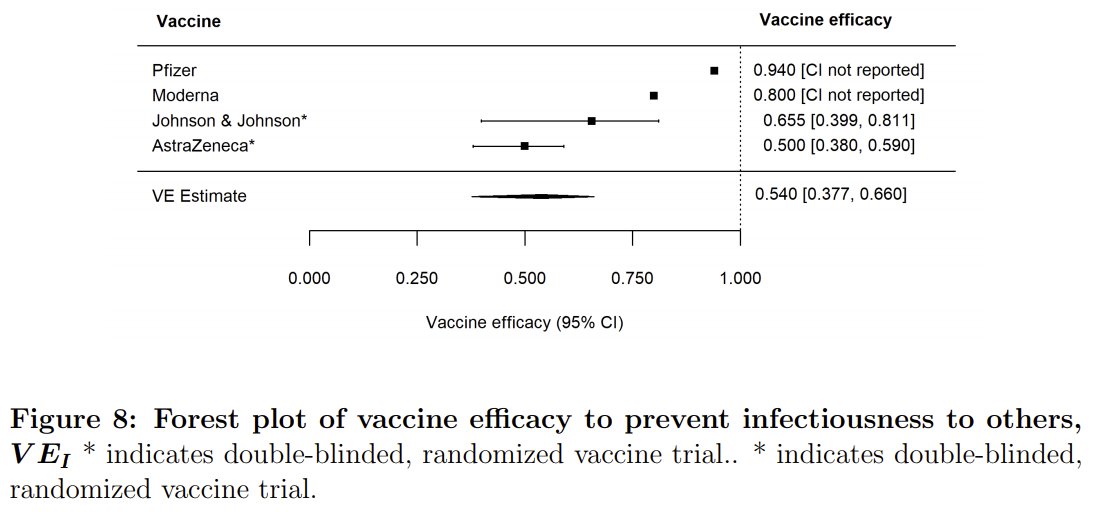
infectiousness 54% (38-66%), but see below
Protection vs
hospitalization 85% (71-92%)
death (no overall estimate)
all infection 83.9% (70-91%)
infectiousness 54% (38-66%), but see below
Finally, Variants: protection vs all symptomatic disease:
B.1.1.7 86% (65 - 84%)
P.1: 61% (43-73%)
B.1.351: 56% (29 - 73%)
All lower than for non-variants, but efficacy vs severe disease *might* be higher (it was for Pfizer for 351: DOI: 10.1056/NEJMc2104974).
B.1.1.7 86% (65 - 84%)
P.1: 61% (43-73%)
B.1.351: 56% (29 - 73%)
All lower than for non-variants, but efficacy vs severe disease *might* be higher (it was for Pfizer for 351: DOI: 10.1056/NEJMc2104974).

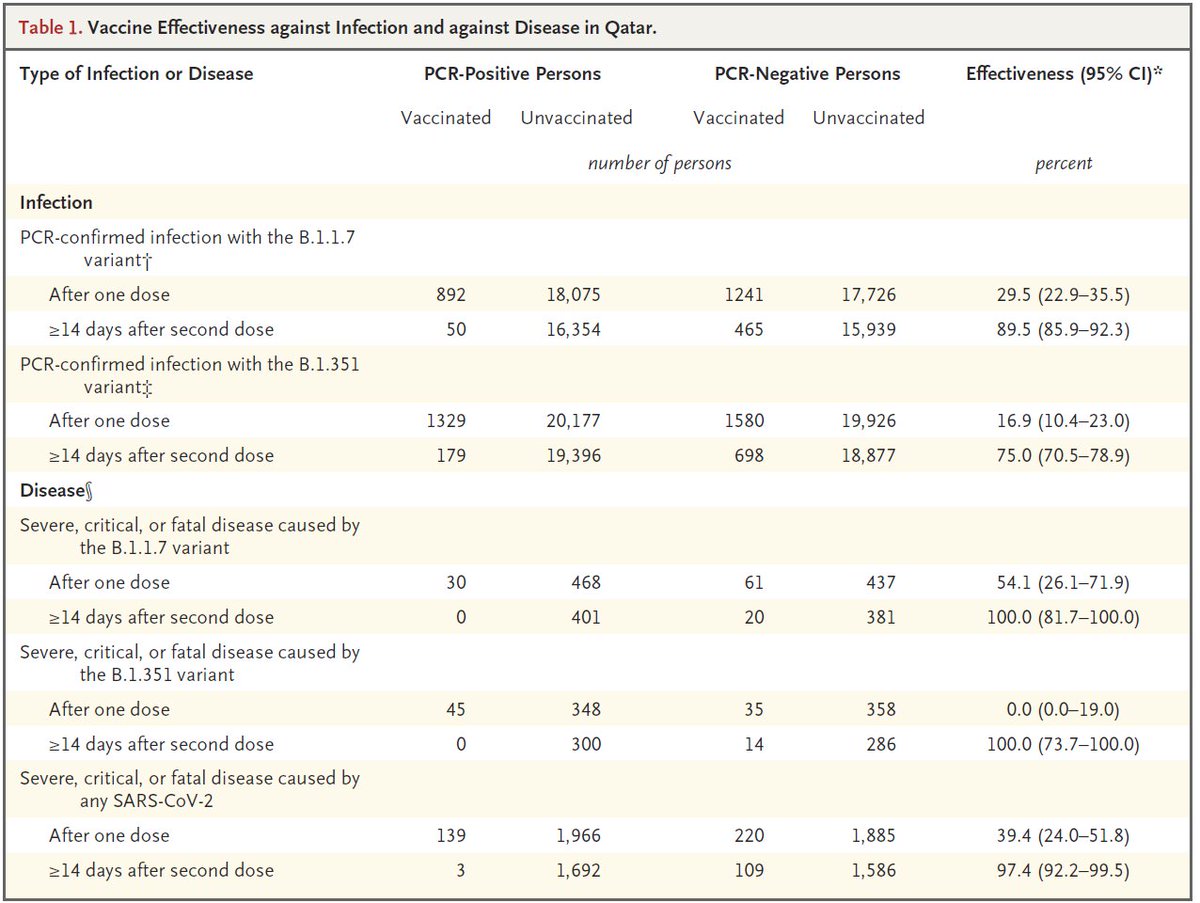
Authors make strange statement that efficacy for B.1.1.7 is a little lower, but doesn't have mutation that affects immunity. This is an oxymoron, & is inconsistent w/ ~2x neutralizing antibody data: Table 9. Immune escape of B.1.1.7 is lower than B.1.351 but not completely absent

Overall, it's a very nice collection of evidence showing very strong protection from vaccines. A few things were less than ideal, that I hope authors will revise.
-Protection against severe infection/death/hospitalization for most vaccines was shown as 100% w/ no CI given. But most (all?) of these studies provide data (N each group, exposure days) to estimate a crude CI even if it wasn't given in study.
This matters a ton b/c efficacy vs most severe forms are high, but obviously not 100%. Thus, the lower 95% CI is of substantial interest, but isn't given for any of these measures & no overall estimate.
Second, estimates of reduction in infectiousness were strange to me. J&J estimate is based on serology not viral loads or attack rates. If so, isn't it estimate of protection vs all infection, not infectiousness? What am I missing? Same for some other estimates in Table 8.
I think it would also have been helpful to include studies on reduction in viral load & map those to infectiousness using several studies now available (e.g.
https://twitter.com/DiseaseEcology/status/1359213763199598594). It appears one of their estimates is based on this?
Good: Authors note they will be updating dataset.
Not so good: It'd be great if data could be shared in a freely accessible data file (e.g. on a github page). Instead, paper doesn't even include data file w/ preprint. That seems very strange to me.
Not so good: It'd be great if data could be shared in a freely accessible data file (e.g. on a github page). Instead, paper doesn't even include data file w/ preprint. That seems very strange to me.
I couldn't figure out how authors did some of their calculations to generate estimates not reported in original sources that were mentioned in Figure/Table legends. A longer methods section would be appreciated.
Tiny unimportant details (but worth addressing):
-Isn't data on protection from RCTs "efficacy" whereas from observational studies it's "effectiveness"? Paper calls everything "efficacy".
-there are several typos in abstract
-Isn't data on protection from RCTs "efficacy" whereas from observational studies it's "effectiveness"? Paper calls everything "efficacy".
-there are several typos in abstract
Worth linking to another recent review, just published, with overlapping datasets on vaccine protection vs infection/transmission: @mugecevik @AaronRichterman @EricMeyerowitz
academic.oup.com/ofid/advance-a…
academic.oup.com/ofid/advance-a…
Some folks likely interested in this:
@joel_c_miller @AdamJKucharski @mlipsitch @CT_Bergstrom @Bob_Wachter
@joel_c_miller @AdamJKucharski @mlipsitch @CT_Bergstrom @Bob_Wachter
• • •
Missing some Tweet in this thread? You can try to
force a refresh