A fab 🧵 to help you get out of bed!
1/
6/21 - bit.ly/2TbybKM #cpsvmrpearls The Ddx for lymphocytic pleocytosis is divided into Infectious causes (bacterial, viral, parasitic, fungi) and Non-Infectious causes (Autoimmune and Malignancy)
1/
6/21 - bit.ly/2TbybKM #cpsvmrpearls The Ddx for lymphocytic pleocytosis is divided into Infectious causes (bacterial, viral, parasitic, fungi) and Non-Infectious causes (Autoimmune and Malignancy)

2/
6/22- bit.ly/35Vi32L #cpsvmrpearls We usually think of neurocysticercosis -> seizure or HA w a circle & a dot/few dots on imaging, but there is a rare form called cysticercal encephalitis that is
1. more common in young girls
2. p/w miliary cysticercosis & AMS (1/2)
6/22- bit.ly/35Vi32L #cpsvmrpearls We usually think of neurocysticercosis -> seizure or HA w a circle & a dot/few dots on imaging, but there is a rare form called cysticercal encephalitis that is
1. more common in young girls
2. p/w miliary cysticercosis & AMS (1/2)
In these pts., remember to avoid anti-parasitic drugs which can cause fatal cerebral edema
Tx = steroids & AEDs (2/2)
Tx = steroids & AEDs (2/2)

3/
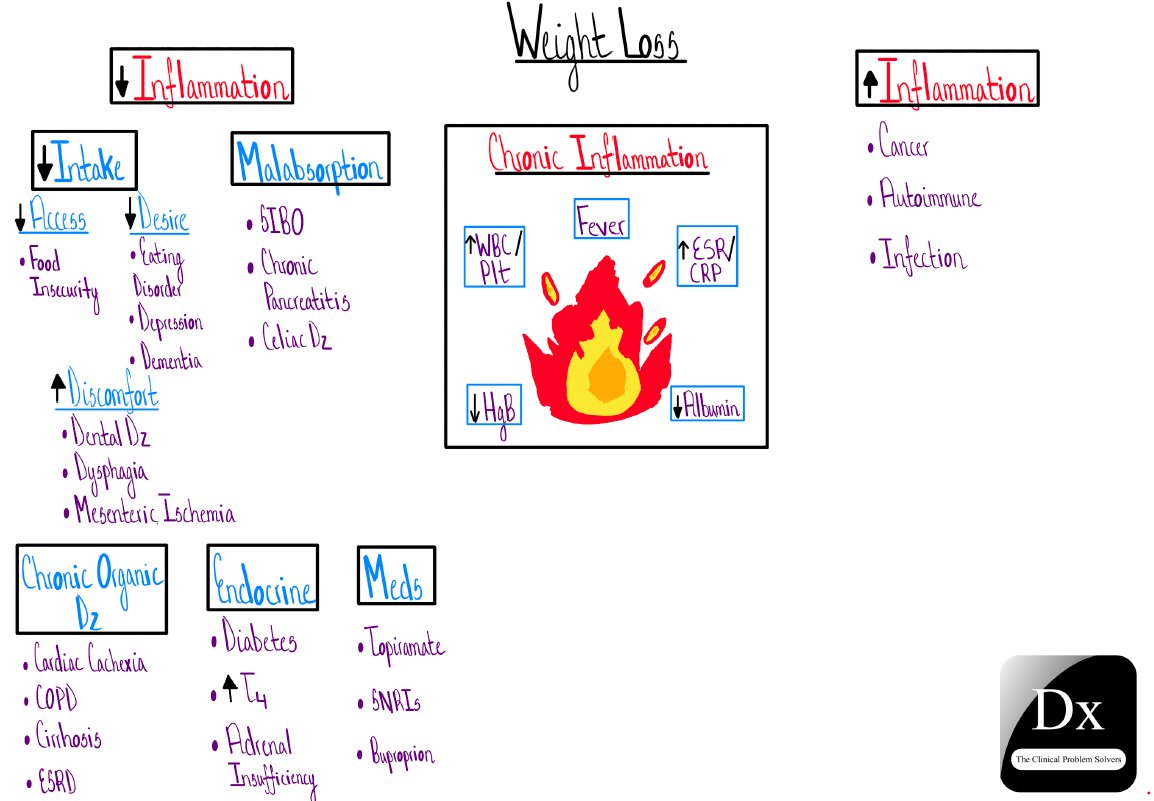
6/23 - bit.ly/3x0OCbF #cpsvmrpearls Thrombocytopenia can be interpreted as an acute phase reactant, whereas thrombocytosis suggests chronic inflammation.
6/23 - bit.ly/3x0OCbF #cpsvmrpearls Thrombocytopenia can be interpreted as an acute phase reactant, whereas thrombocytosis suggests chronic inflammation.
4/
6/24 - bit.ly/2Sw2rj7 #cpsvmrpearls Acute pericalcific arthritis mimics Septic arthritis and Crystalline arthropathies.
6/24 - bit.ly/2Sw2rj7 #cpsvmrpearls Acute pericalcific arthritis mimics Septic arthritis and Crystalline arthropathies.


6/
6/27 - #cpsvmrpearls Amyloidosis can affect the GI tract causing protein losing enteropathy and therefore anasarca.
6/27 - #cpsvmrpearls Amyloidosis can affect the GI tract causing protein losing enteropathy and therefore anasarca.


• • •
Missing some Tweet in this thread? You can try to
force a refresh