1/ #MedTwitter, we have another lactic acidosis case!
Find the last two here:
(1) bit.ly/33gz9pu
(2) bit.ly/2U95Ktm
You just placed a pt on precaution for COVID & get a page about your next admission...
56M p/w R leg pain 1 hr after injuring his shin at home.
Find the last two here:
(1) bit.ly/33gz9pu
(2) bit.ly/2U95Ktm
You just placed a pt on precaution for COVID & get a page about your next admission...
56M p/w R leg pain 1 hr after injuring his shin at home.
2/ T 99F, BP 127/78, HR 84, R 13, 98%
The R leg is bruised, swollen, and tender.
X-ray was w/o fracture, but U/S showed a large hematoma in the anterior R lower leg.
Patient reports frequent nosebleeds & bruising during the past year. Denies a FHx of bleeding conditions.
The R leg is bruised, swollen, and tender.
X-ray was w/o fracture, but U/S showed a large hematoma in the anterior R lower leg.
Patient reports frequent nosebleeds & bruising during the past year. Denies a FHx of bleeding conditions.
3/ Labs:
Hgb 11
PLT 220
Blood smear - normal
BMP - normal
aPTT 99 (25-36)
PT 12 (10-13)
Fibrinogen 300
Plasma vWF antigen - normal
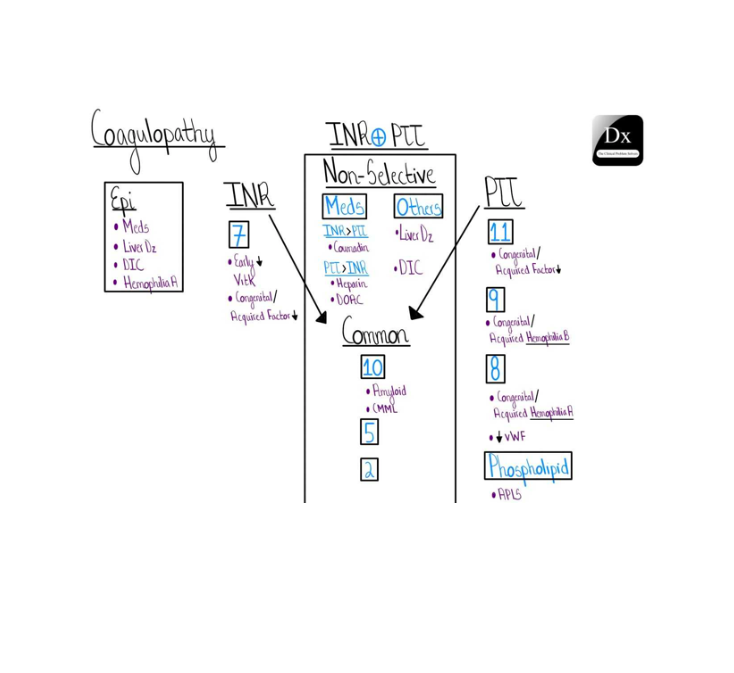
Need a bit of a refresher on coagulation studies? Luckily, @CPSolvers is working on a schema for you! #MedTwitter, we’d appreciate your feedback!
Hgb 11
PLT 220
Blood smear - normal
BMP - normal
aPTT 99 (25-36)
PT 12 (10-13)
Fibrinogen 300
Plasma vWF antigen - normal
Need a bit of a refresher on coagulation studies? Luckily, @CPSolvers is working on a schema for you! #MedTwitter, we’d appreciate your feedback!
4/ After confirming no exposure to heparin, you send a mixing study.
Over the next 3h, the patient’s pain gets worse. His leg is tense but warm, with intact distal pulses. He jumps when you plantar flex his foot.
Lactic acid is 4.6. Let’s review causes of lactic acidosis!
Over the next 3h, the patient’s pain gets worse. His leg is tense but warm, with intact distal pulses. He jumps when you plantar flex his foot.
Lactic acid is 4.6. Let’s review causes of lactic acidosis!

5/ You call surgery, who measures the compartment pressure to be 43 mmHg (nl < 30). Compartment syndrome (CS) is diagnosed, and a fasciotomy is performed.
Nice work! Let’s review some teaching points about CS!
We learned a great deal from @DissanaikeMD!
Nice work! Let’s review some teaching points about CS!
We learned a great deal from @DissanaikeMD!
6/ CS occurs when an anatomical compartment has an increase in pressure, impairing circulation. This hypoperfusion leads to a lactic acidosis. CS often occurs with crush injuries but can happen from mild trauma in patients with bleeding disorders.
What have you seen cause CS?
What have you seen cause CS?
7/ Early signs to look out for are:
1) Pain out proportion to exam
2) Pain with passive flexion
Other signs, such as weakness, numbness, pallor, and pulselessness are not sensitive, often occur in the late stage, and should not be used to rule out the condition.
1) Pain out proportion to exam
2) Pain with passive flexion
Other signs, such as weakness, numbness, pallor, and pulselessness are not sensitive, often occur in the late stage, and should not be used to rule out the condition.
8/ A normal initial pressure measurement does not rule out compartment syndrome. Instead, the measurements should be trended over time and correlated clinically.
Acute compartment syndrome is a surgical emergency, and time = muscle!
Acute compartment syndrome is a surgical emergency, and time = muscle!
9/ Since no finding is 100% sensitive/specific, diagnosis requires a high clinical suspicion. Management involves:
1) Removal of any external constriction (casts, bandages)
2) Correcting hypotension (with IVF)
3) Early surgical consultation
1) Removal of any external constriction (casts, bandages)
2) Correcting hypotension (with IVF)
3) Early surgical consultation
10/ After the fasciotomy, the patient has prolonged bleeding.
The mixing study does not correct the aPTT.
Lupus anticoagulant is excluded.
Factor VIII activity returns <30%
A Bethesda assay returns at 5 BU/mL consistent with acquired hemophilia A due to a high titer inhibitor.
The mixing study does not correct the aPTT.
Lupus anticoagulant is excluded.
Factor VIII activity returns <30%
A Bethesda assay returns at 5 BU/mL consistent with acquired hemophilia A due to a high titer inhibitor.
11/ The patient is treated with recombinant factor VIII. Autoimmune + age related malignancy workup is pursued.
Final diagnosis: compartment syndrome due to hematoma in a patient with acquired hemophilia A.
Thanks for following along with us!
Final diagnosis: compartment syndrome due to hematoma in a patient with acquired hemophilia A.
Thanks for following along with us!