1/ Our paper on pre- and post ejection tissue velocities by #EchoFirst in relation to valve closures and openings is out: onlinelibrary.wiley.com/doi/epdf/10.11…
2/ 22 healthy subjects, Valve openings and closures timed by Doppler flow, and transewfrred to Tissue Doppler recordings. 

3/ Pre ejection velocities started 24.8 ms after start QRS, with a duration of 51.5 ms, ending about 11.5 ms after MVC. Thus, both electromechanical delay and pre ejection velocity occurs *before* onset of IVC, and are not a measure of IVC or Isovolumic acceleration.

4/ This has been shown by ultra high frame rate imaging previously. So what is the significance of the pre ejection velocities? It's not recoil from atrial relaxation, as it's present in fib, and absent in AV-block. pubmed.ncbi.nlm.nih.gov/24210859/
5/ Both initial pressure increase pubmed.ncbi.nlm.nih.gov/623315/ and volume decrease pubmed.ncbi.nlm.nih.gov/18606917/ occurs before MVC, indicating that the pre ejection velocities are active contraction. The latter reference has shown it also by stenting the MV.
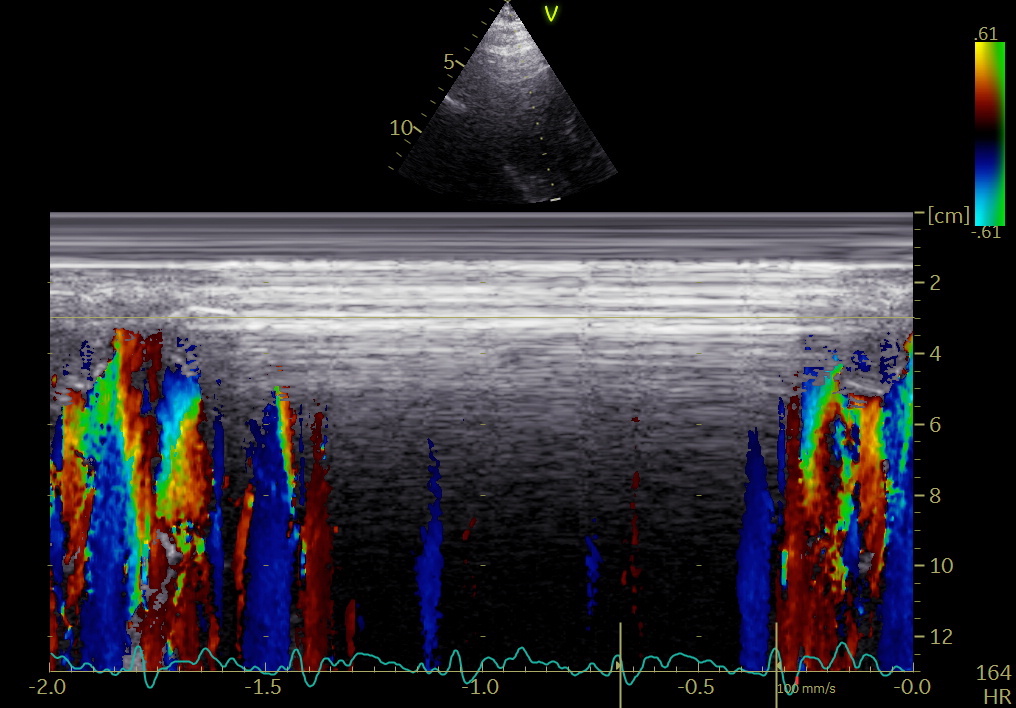
6/ In the present study, we show the active shortening by strain rate. Thus, this seems to be the marker of electromechanic activation, which is simultaneous in septum and the lateral wall, possibly by left anterior and left posterior bundle.

7/ This has been shown previously: electrical breakthrough simultaneous in septum and laterally pubmed.ncbi.nlm.nih.gov/6723010/ , and with an electromechanical delay of about 20 - 30 ms pubmed.ncbi.nlm.nih.gov/14670817/ , in line with our study: 25 ms from onset Q to onset pre ejection spike
8/ But what is then the significance of the pre ejection contraction?
-firstly, a small volume reduction, as seen by mitral annulus displacement. Not due to ejection, but exclusion of the volume by the annulus.
-firstly, a small volume reduction, as seen by mitral annulus displacement. Not due to ejection, but exclusion of the volume by the annulus.

9/ - Secondly, as the annulus moves in a stationary blood column, the leaflets will be pushed towards closure, possibly in combination by the last of the filling vortex, so pre ejection contraction is part of the mechanism for MVC.
10/ -Thirdly, the apical motion will stop at the closure of the MV, which is the start of the real IVC. Including the pre ejection spike in IVC will over estimate IVC by about 40 ms, and including EMD as well, will over estimate IVC by further 25ms.
11/ There is no ring motion during IVC, LV being isovolumic, and concepts like IVC velocity or acceleration are erroneous. Start ejection is at AVO, when LV and Ao pressures are equalised, the start of ring motion during ejection is, of course simultaneous in all parts
12/ -and the onset of the main shortening event, is the end of IVC/AVO, and certainly not electromechanical activation.

• • •
Missing some Tweet in this thread? You can try to
force a refresh