
1/ Our preprint on #SARSCoV2 infection & transmission in secondary schools following the emergence of the Alpha variant in England is now online
We took multiple blood samples from ~2,000 students/staff for #SARSCoV2 antibodies. Here’s what we found 🧵
👉medrxiv.org/content/10.110…
We took multiple blood samples from ~2,000 students/staff for #SARSCoV2 antibodies. Here’s what we found 🧵
👉medrxiv.org/content/10.110…
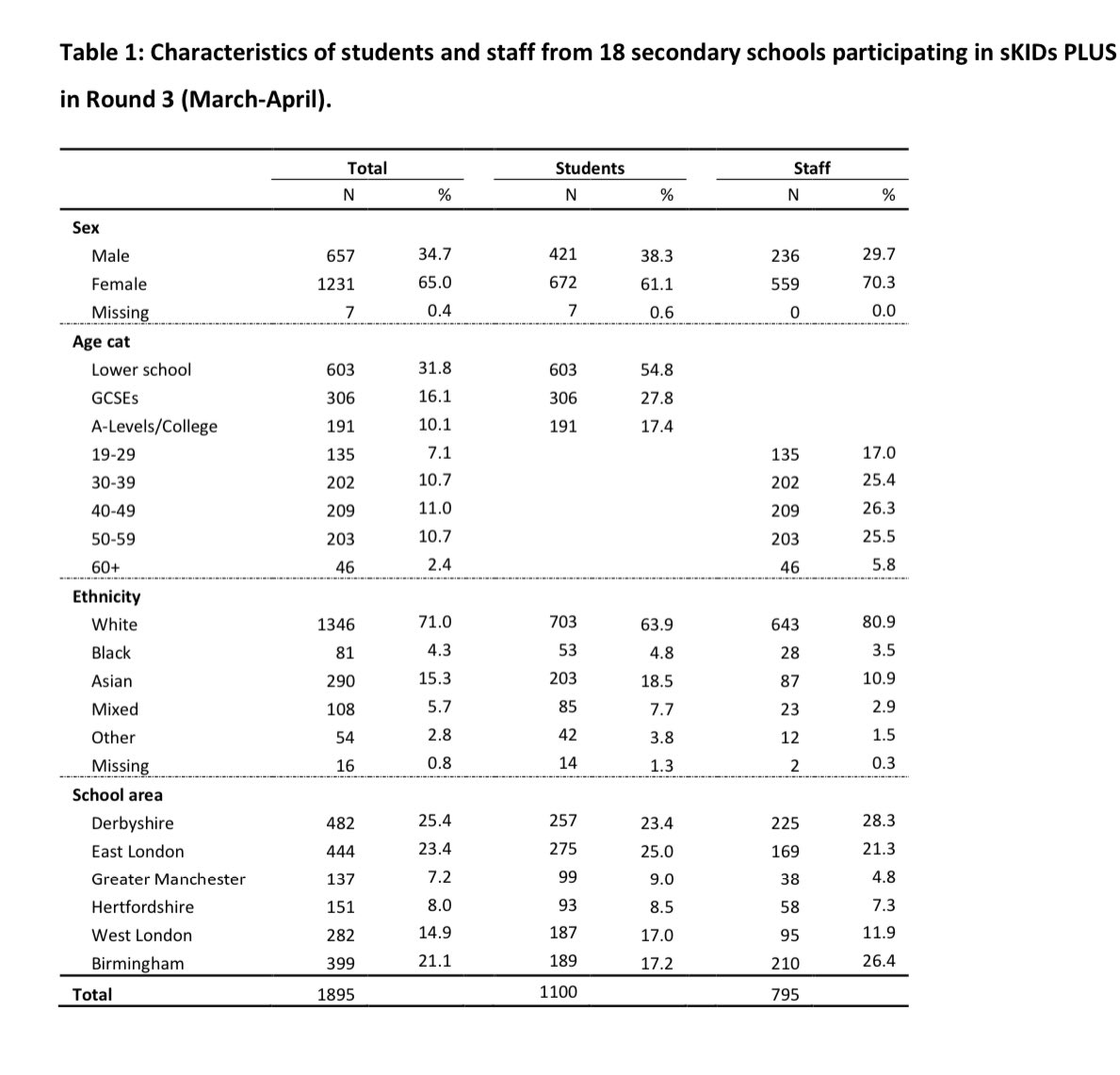
2/ In England, #Covid19 cases due to the Alpha variant increased rapidly from late Nov 2020, leading to national lockdown in Dec 2020, including school closures. When schools reopened fully in Mar 2021, we took blood samples from 1,895 students & staff in our sKIDsPLUS study 
3/ Between December 2020 & March 2021, 5.6% (61/1094) students & 4.4% (35/792) staff had laboratory-confirmed SARS-CoV-2 infection.
Most of these infections were acquired during community peaks in infections rates in December 2020, with a trickle of cases throughout lockdown
Most of these infections were acquired during community peaks in infections rates in December 2020, with a trickle of cases throughout lockdown
4/ Over the same period (median 16 weeks, ~4 mths), 15% (97/656) of students & 10% (59/590) of staff seroconverted (antibody -ve ➡️+ve; captures asymptomatic infections too)
👉 there were 2-3 times as many students/staff with antibody evidence of infection vs PCR-testing alone
👉 there were 2-3 times as many students/staff with antibody evidence of infection vs PCR-testing alone

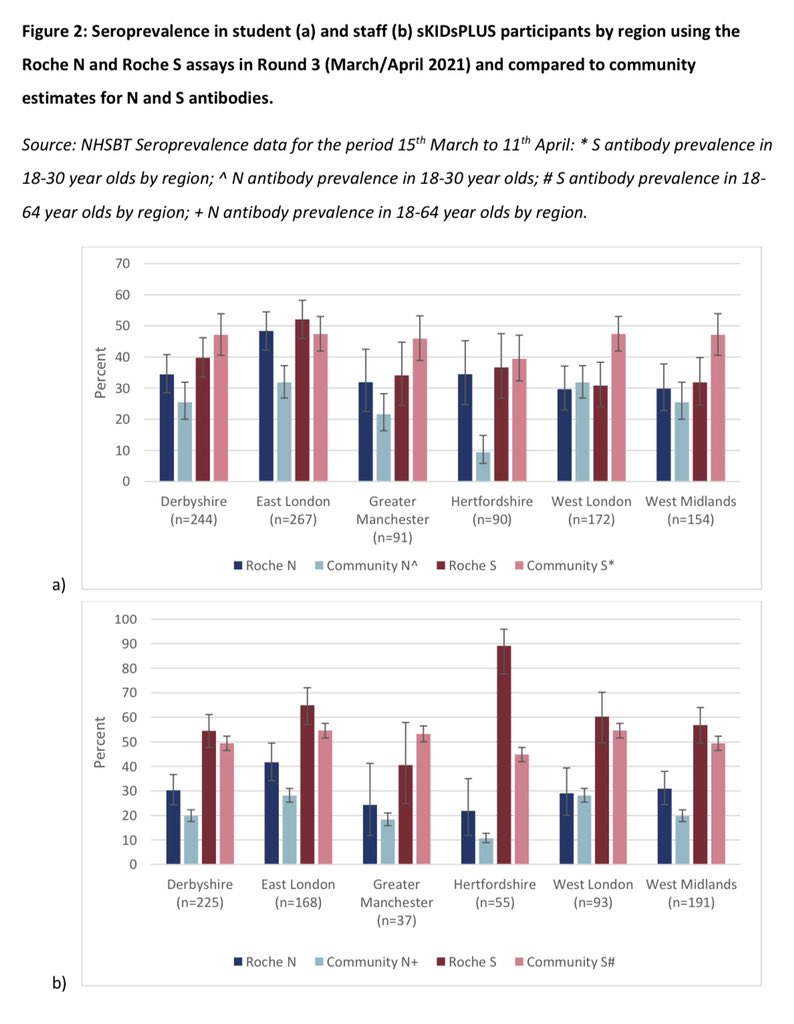
5/ The proportion with evidence of previous infection (Nucleoprotein (N) antibody positive) in March 2021 was 36% (370/1018) in students & 32% (245/769) in staff, but was as high as 50% in some London schools
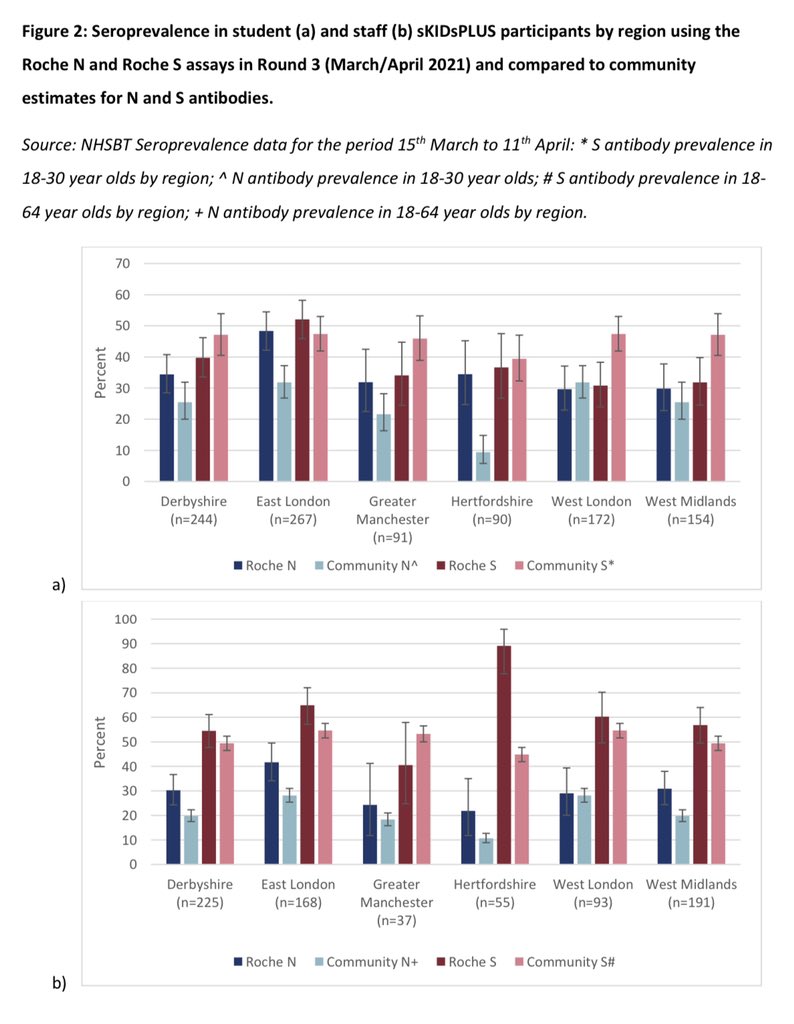
6/ The proportion with spike protein (S) antibodies (due to infection and/or vaccine) was 40% (402/1018) is students & 60% (459/769) in staff, similar to regional community seroprevalence. Staff had higher proportion with Spike protein antibody because of vaccination
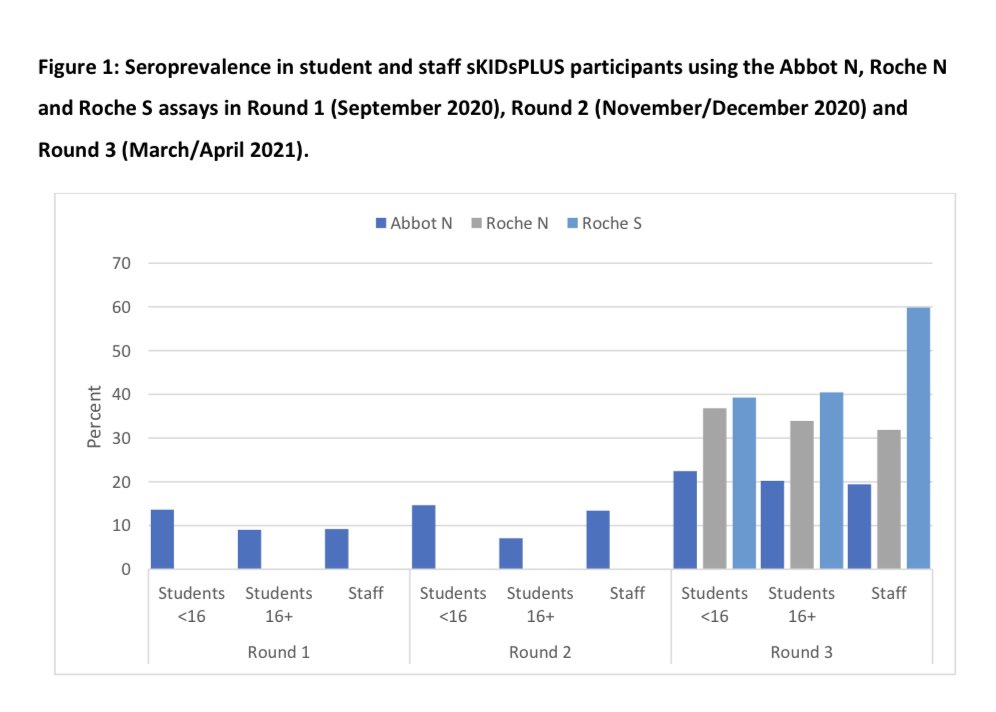
7/ For the unbelievers of #SARSCoV2 antibodies as a marker of infection, we used multiple antibody testing platforms & showed that the Roche N and S assays were the most reliable, while the Abbott N assay had uncharacteristically high antibody decay rates over time (assay effect)
8/ To conclude:
By March 2021, 1 in 3 students in urban secondary schools had serological evidence of #SARSCoV2 infection (up to 50% in London)
👉antibody rates likely higher now after Delta variant
👉these findings are important when considering vaccination of teenagers
End
By March 2021, 1 in 3 students in urban secondary schools had serological evidence of #SARSCoV2 infection (up to 50% in London)
👉antibody rates likely higher now after Delta variant
👉these findings are important when considering vaccination of teenagers
End
• • •
Missing some Tweet in this thread? You can try to
force a refresh








