
🚨New #OpenAccess Article 🚨
New review article highlighting key points in fluid resuscitation for septic patients, on the wards or perhaps on the verge of needing ICU.
I admit, not without agenda (⬇️fluid overload)
Freely available through Sept 2: sciencedirect.com/science/articl…
New review article highlighting key points in fluid resuscitation for septic patients, on the wards or perhaps on the verge of needing ICU.
I admit, not without agenda (⬇️fluid overload)
Freely available through Sept 2: sciencedirect.com/science/articl…


A few editorial points:
Most of the evidence presented involves critically ill patients, but the lessons shouldn’t much differ if you have a hypotensive/malperfused patient on the wards.
Without the benefit of vasopressors, it’s difficult to determine how to safely resuscitate
Most of the evidence presented involves critically ill patients, but the lessons shouldn’t much differ if you have a hypotensive/malperfused patient on the wards.
Without the benefit of vasopressors, it’s difficult to determine how to safely resuscitate
We advocate for a hemodynamically-targeted approach to fluid resuscitation. It’s difficult to assess fluid responsiveness in the ICU, moreso on the wards.
(Proposed approach, not prospectively validated)
(Proposed approach, not prospectively validated)

Given potential harms of fluid overload, this is a situation to consider early ICU transfer rather than continued boluses that the patient “seems” to respond to briefly.
As intensivists, we need to be better advocates for patients in this situation, as well as their team
As intensivists, we need to be better advocates for patients in this situation, as well as their team
Once upon a time (or currently in some places), a patient needed to “prove” their need for ICU by having received extensive fluid loading.
Hopefully we are moving out of this paradigm
Hopefully we are moving out of this paradigm
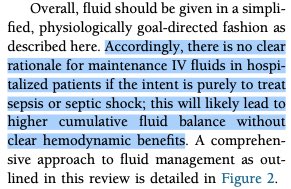
To this point, maintenance fluids in wards patients without ongoing fluid losses ought to be avoided.
I’m sure this work will generate some strong opinions, but overall we feel this is a good starting point for reconsideration of fluid management in septic patients on the wards.
Tempted to tag many hospitalist friends, but I’d rather you discover it on your own!
Tempted to tag many hospitalist friends, but I’d rather you discover it on your own!
• • •
Missing some Tweet in this thread? You can try to
force a refresh










{kind=link}