For those asking when this is going to end:
Once >6 mo kids can get vaxxed, then only those with weaker immunity need boosters on occasion. <6mo old would count on lower prevalence to reduce risk
What we could really use: greek alphabet soup vaccines
nytimes.com/2021/08/18/hea…
Once >6 mo kids can get vaxxed, then only those with weaker immunity need boosters on occasion. <6mo old would count on lower prevalence to reduce risk
What we could really use: greek alphabet soup vaccines
nytimes.com/2021/08/18/hea…
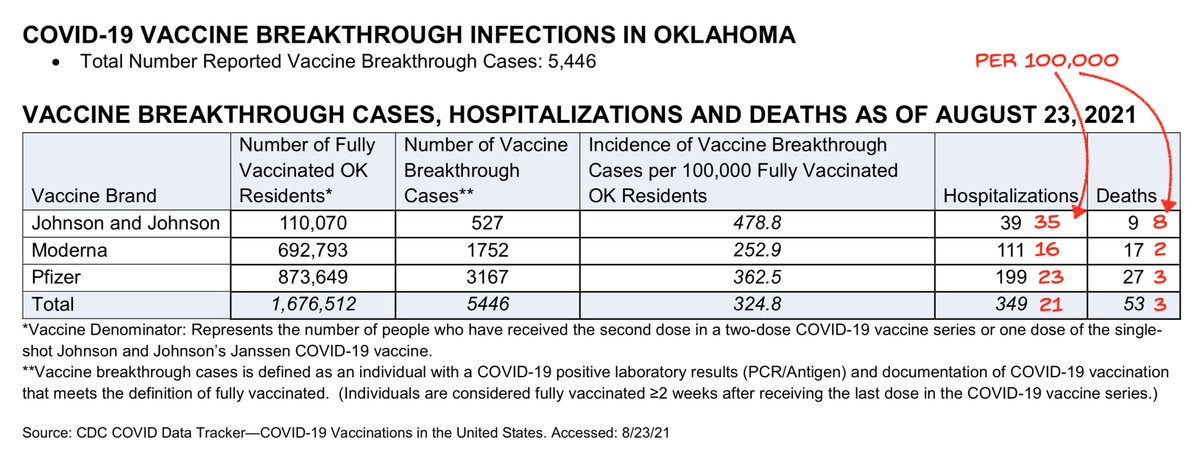
For #JnJers, working on bringing some attention to the issue
Record-number of eye-rolling comments in this article: nytimes.com/2021/08/18/hea…
“Feeling sick like a dog and laid up in bed, but not in the hospital with severe Covid, is not a good enough reason,” Dr. Gounder said.
“Feeling sick like a dog and laid up in bed, but not in the hospital with severe Covid, is not a good enough reason,” Dr. Gounder said.
How about protecting your unvaccinated kids or your elderly (yes even vaccinated) parent this winter? Would that be good enough? Not everybody has selfish reasons here.
Dr. Hanage: “A third shot will add to skepticism among people yet to receive one dose that the vaccines help them.”
100% wrong. Public health officials revising recommendations shows they adapt to the situation, which engenders confidence that policy is up to date.
100% wrong. Public health officials revising recommendations shows they adapt to the situation, which engenders confidence that policy is up to date.
Just amazing that some people still insist that vaccines must be spoken of as perfect, even if it means completely changing their definition of perfect along the way. If you stick to argument by shifting your reasons and definitions, it is you who loses credibility.
Not sure if anybody noticed the own-goal: 'But not all immunocompromised persons will respond to an additional dose of vaccine,” Dr. Gounder noted. To protect these vulnerable individuals, everyone around them should be vaccinated and should continue to wear masks, she added.'
Let's see... immunocompromised may still not mount a great response to the booster (although studies show some do, definitely a net gain). So those around them need to be vaccinated! But didn't she just say the vaccinated should be okay with getting sick (and contagious)?
"We never meant unsinkable to mean it wouldn't sink. The ship still has efficacy as a habitat for sea creatures, so it does what we expected it to do eventually."
"If we now boost the number of lifeboats on the Olympic, it might add to skepticism among the people who have never been on a ship before. Better to say everything has been working as designed. After all Titanic did keep people dry more than halfway across."
I'm clearly not getting a job in public health after this
Okay this analogy has legs
"Our unsinkable guidance was based on evidence of Titanic floating and lack of evidence otherwise. New science we have today suggests that on occasion this design can sink. But we shouldn't add lifeboats to Olympic as it may add to hesitancy to sail."
"Our unsinkable guidance was based on evidence of Titanic floating and lack of evidence otherwise. New science we have today suggests that on occasion this design can sink. But we shouldn't add lifeboats to Olympic as it may add to hesitancy to sail."
• • •
Missing some Tweet in this thread? You can try to
force a refresh