
1) There was an ACIP meeting today, but nothing newsworthy happened. CDC briefing materials (as posted at cdc.gov/vaccines/acip/…) are limiting the ability of ACIP to independently and intelligently assess data.
2) Most concerning, CDC continues to withhold J&J data by omitting it entirely or lumping it together with the 10x larger Pfizer+Moderna data so it becomes a rounding error. No wonder ACIP is not able to make any recommendations specifically for J&J
cdc.gov/vaccines/acip/…
cdc.gov/vaccines/acip/…


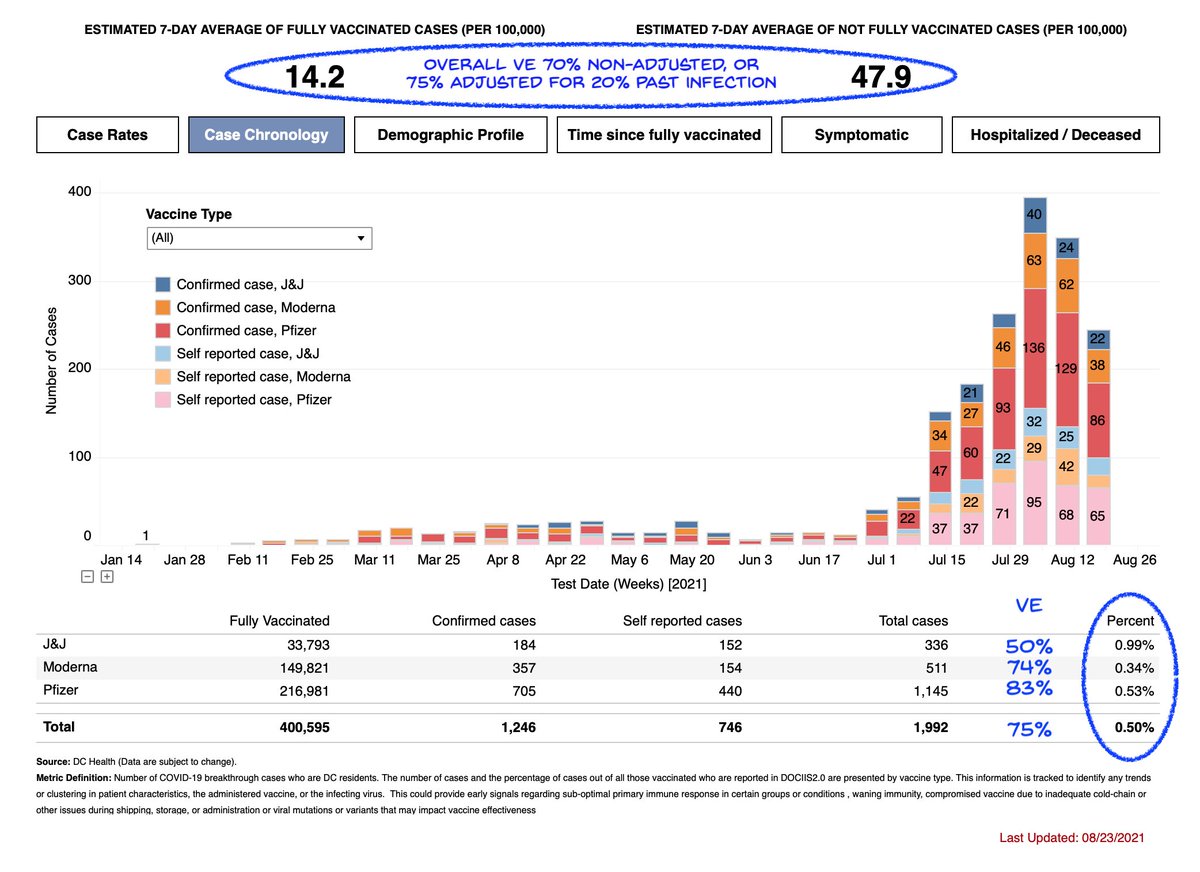
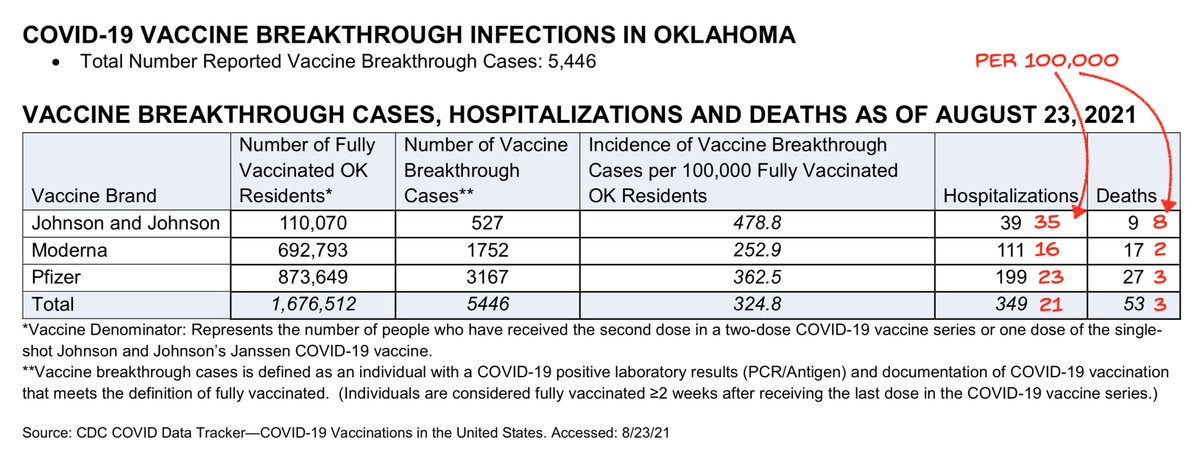
3) But the data exist, and is becoming increasingly in plain sight, showing higher case and hospitalization rates for J&J than for Pfizer and Moderna in the real world against Delta
4) Also there was no discussion of how boosters may be useful beyond the boosted individual. Most disappointingly, there was no raising of the question of mixing boosters.
ACIP will only address the questions CDC asks them, but CDC is leaving out some very important ones.
ACIP will only address the questions CDC asks them, but CDC is leaving out some very important ones.
• • •
Missing some Tweet in this thread? You can try to
force a refresh





