As the evidence supporting ivermectin as COVID treatment collapses, you might expect *less* certainty from the drug’s evangelists.
Instead they’ve doubled down on ivermectin.
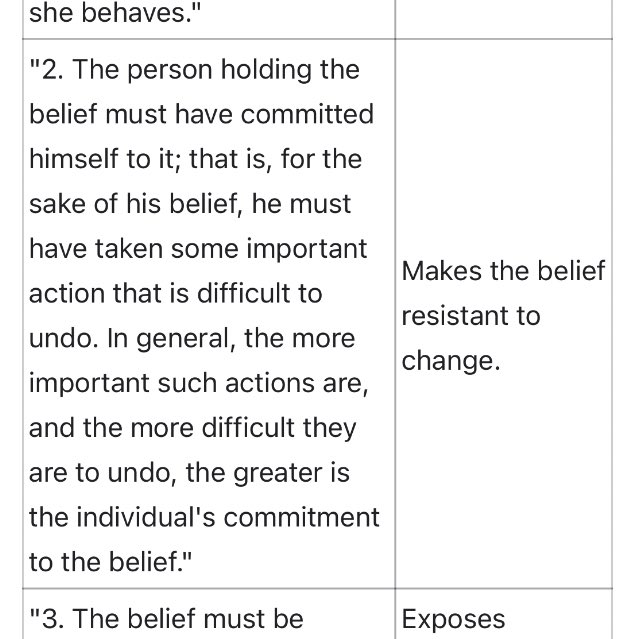
It’s worth reading this passage from Festinger’s Theory of Cognitive Dissonance to understand:
1/
Instead they’ve doubled down on ivermectin.
It’s worth reading this passage from Festinger’s Theory of Cognitive Dissonance to understand:
1/


For context, Festinger & colleagues joined a cult (“The Seekers”) who believed the world would end on December 21, 1954 & that true believers would be rescued by a UFO
The researchers wondered how the Seekers would react to “disconfirmation” when this didn’t happen.
2/
The researchers wondered how the Seekers would react to “disconfirmation” when this didn’t happen.
2/
As the date approached, the researchers watched many “Seekers” take irrevocable steps because of their belief: they quit their jobs, severed ties to loved ones, & disposed of possessions.
What would happen when their beliefs were discredited?
3/
What would happen when their beliefs were discredited?
3/


When 12/21/54 came and went without the promised apocalypse, they observed that rather than abandoning their discredited beliefs, the “Seekers” adhered to them even *more strongly* & began to proselytize *more fervently*.
4/
4/

Examining the Seekers & other examples, Festinger & colleagues theorized that in order to resolve the dissonance between belief & reality, believers sometimes become more fervent in their belief (discounting reality).
They observed 5 conditions that make this more likely:
5/
They observed 5 conditions that make this more likely:
5/

Now consider the experience of ivermectin believers:
- many of the initial studies supporting IVM have been discredited as fraudulent (Surgisphere, Elegazzar, Cadegiani)
- several large RCTs have found no benefit to IVM (EPIC, TOGETHER, IVERCORCOVID)
6/
nature.com/articles/d4158…
- many of the initial studies supporting IVM have been discredited as fraudulent (Surgisphere, Elegazzar, Cadegiani)
- several large RCTs have found no benefit to IVM (EPIC, TOGETHER, IVERCORCOVID)
6/
nature.com/articles/d4158…
- a reputable meta-analysis by Cochrane (the gold standard) concluded “the reliable evidence available does not support the use of ivermectin for treatment or prevention of COVID‐19”
7/
cochranelibrary.com/content?templa…
7/
cochranelibrary.com/content?templa…
- multiple state & federal agencies (FDA, CDC, NIH, etc) have warned people explicitly NOT to take ivermectin
- the rampant use of veterinary ivermectin has led to a surge in poisonings. (Last week >70% of calls to poison control center in MS were about ivermectin)
8/
- the rampant use of veterinary ivermectin has led to a surge in poisonings. (Last week >70% of calls to poison control center in MS were about ivermectin)
8/
https://twitter.com/US_FDA/status/1429050070243192839

- And finally, the rapid development of safe, highly effective, & widely available vaccines has eliminated the raison d'être of IVM as a “bridge to vaccines”
In light of all this evidence “disconfirming” IVM, why do its proponents cling to it all the more fervently?
9/
In light of all this evidence “disconfirming” IVM, why do its proponents cling to it all the more fervently?
9/
If we look at Festinger’s 5 conditions, we can see that all are met:
1. The core believers (FLCCC, BIRD, etc) are deeply & publicly committed to this belief. One has testified before Congress that IVM is a “wonder drug” & “miracle cure.” Others have built a brand on IVM.
10/
1. The core believers (FLCCC, BIRD, etc) are deeply & publicly committed to this belief. One has testified before Congress that IVM is a “wonder drug” & “miracle cure.” Others have built a brand on IVM.
10/

2. Believers in IVM have invested all of their reputation in the belief. Most have lost the respect of colleagues. At least one has stopped practicing medicine to focus exclusively on promoting IVM as a cure.
For many it would be hard, or impossible, to undo these effects.
11/
For many it would be hard, or impossible, to undo these effects.
11/
3&4. At least a dozen large high quality RCTs of IVM are ongoing. Each is explicitly testing whether IVM can prevent or treat COVID.
Each can potentially falsify the belief that IVM prevents/cures COVID (and several already have).
12/
Each can potentially falsify the belief that IVM prevents/cures COVID (and several already have).
12/

5. Although some people, confronted by the overwhelmingly negative evidence, have stopped believing in IVM, most have stayed committed to the core belief and the group.
Having invested so much time & reputation, many find it is hard to just walk away.
13/
Having invested so much time & reputation, many find it is hard to just walk away.
13/

The core IVM believers have taken on increasingly anti-vaxx conspiracy theorist beliefs:
- Not only do they discount the mounting negative studies of IVM but they allege a massive global cabal of governments, big tech, & pharma to encourage vaccination and “suppress the cure”
14/
- Not only do they discount the mounting negative studies of IVM but they allege a massive global cabal of governments, big tech, & pharma to encourage vaccination and “suppress the cure”
14/
What will happen?
Faced with “disconfirmation” & increasing cognitive dissonance most cults eventually collapse.
After the world didn’t end on 12/21/54, the “Seekers” rescheduled the apocalypse to Christmas Eve. When 12/25 came & went, most members returned to their lives.
15/
Faced with “disconfirmation” & increasing cognitive dissonance most cults eventually collapse.
After the world didn’t end on 12/21/54, the “Seekers” rescheduled the apocalypse to Christmas Eve. When 12/25 came & went, most members returned to their lives.
15/

I suspect the same will occur with the #CultOfIvermectin
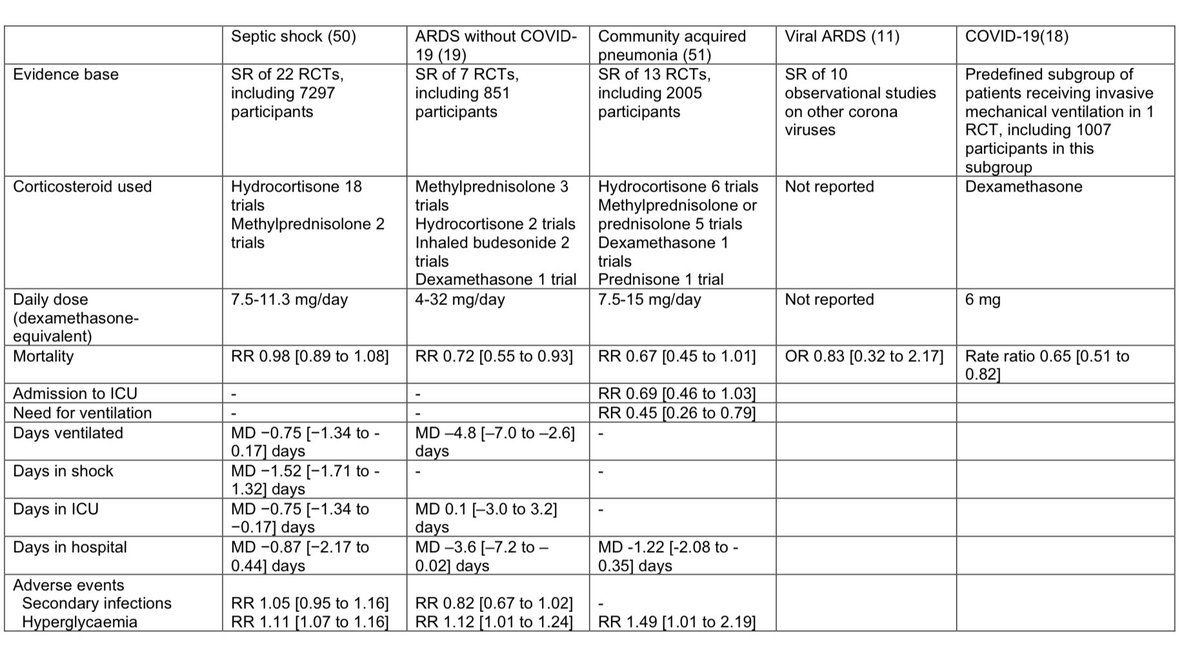
Recall that a founder of FLCCC claimed to have “cured sepsis” a few yrs ago. In light of negative RCTs that cult/belief also collapsed
The question is how many will be harmed along the way?
16/16
pulmccm.org/critical-care-…
Recall that a founder of FLCCC claimed to have “cured sepsis” a few yrs ago. In light of negative RCTs that cult/belief also collapsed
The question is how many will be harmed along the way?
16/16
pulmccm.org/critical-care-…


• • •
Missing some Tweet in this thread? You can try to
force a refresh