Apart from the physiological implications, what are the consequences of this study onlinelibrary.wiley.com/doi/epdf/10.11… for timing of valve openings and closures by tissue Doppler? 

1/ Valve closures can be timed by tissue Doppler and mitral ring motion. However, only the septal motion will reliably show AVC.

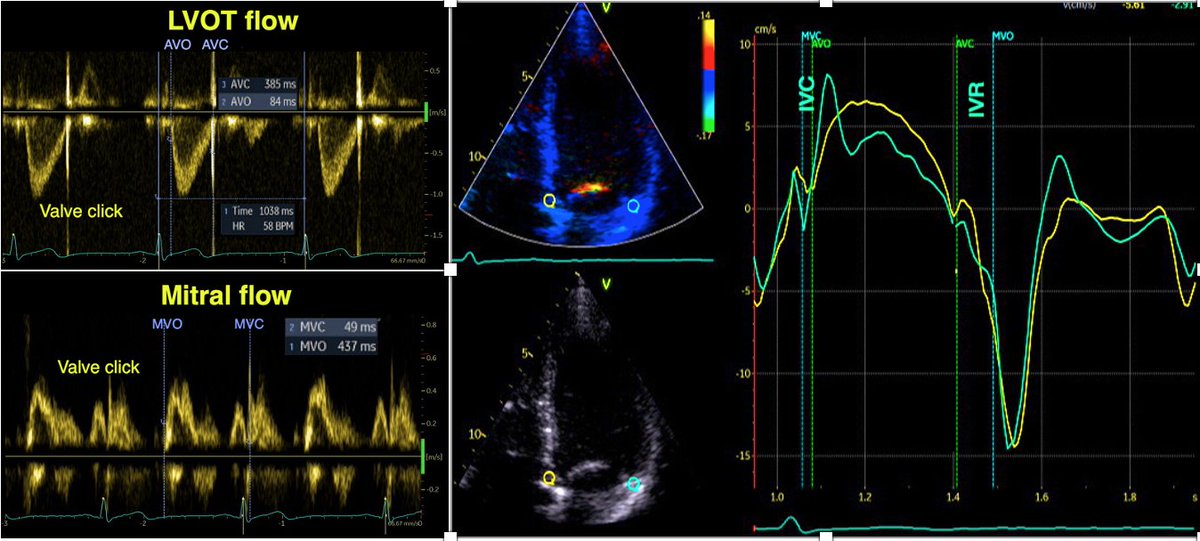
2/ MVO is close to the END of the pre ejection spike. Timing MVC by the start of the pre ejection spike will result in an error of about 40 ms too early. Timing by the peak R wave will result in about the same error.
3/ AVC is closest to the END of the post ejection spike. Timing by the start of the spike will result in about 25 ms too early.
4/ In colour TDI of the mitral ring, pre ejection spike is red (positive), end of this is red-to-blue transition. Post ejection spike is blue (negative), end of this is blue-to-red transition. Again the septum is the most reliable.

5/ As colour transition marks the velocity zero crossing points, they differ a little from the nadir/peaks of the curves. In fact the zero crossing points are the most accurate in determining the valve closures.
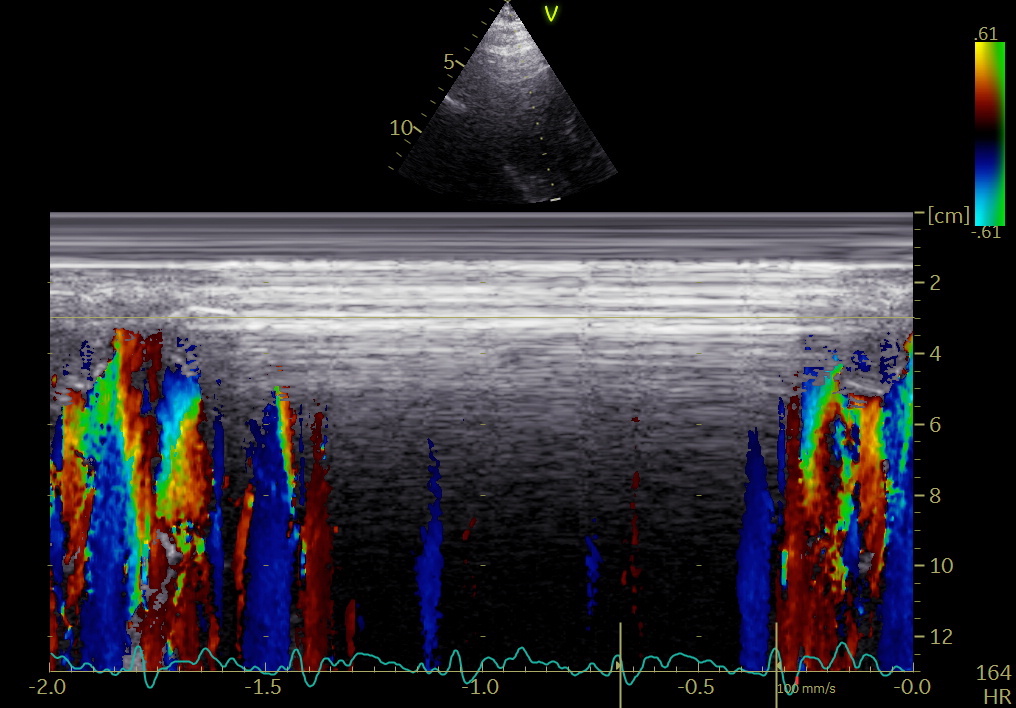
6/ What about the colour M-mode of the anterior mitral leaflet? The mitral leaflet moves together with the mitral ring when MV is closed, but independently during filling.
7/ This means that the pre ejection spike is invisible, being masked by the rapid downward motion of the mitral leaflet, but MVC is excellently visible by the blue-to-red transition of the end of this downward motion.

8/ The short red-to-blue-to-red transition making transition from IVC to ejection, was only visible in about half of the cases, as opposed to all in the septal mitral ring.
8/ the short red-to-blue-to-red transition, marking IVC and the onset of ejection, was limited to about half the cases, both in the mitral ring and leaflet.
9/ The negative post ejection was visible by CAMM in the septal ring in all subjects, but only in half by the mitral leaflet. If present, AVC was the END of this (blue to red transition), cfr. curves, not by the start as maintained previously, the error is about 25 ms.

unroll @threadreaderapp
In this last image, the timing of AVC is evident also from the phonocardiogram, as documented already in 2006 pubmed.ncbi.nlm.nih.gov/16364793/
• • •
Missing some Tweet in this thread? You can try to
force a refresh