
The @Telegraph released an article claiming "we're still not completely sure how coronavirus spreads or how to stop it", muddying the waters re. Airborne Transmission.
If I were a hostile foreign state, with a goal of prolonging the Pandemic in the West, I would write this.
🧵1/
If I were a hostile foreign state, with a goal of prolonging the Pandemic in the West, I would write this.
🧵1/
I'm not surprised that the usual WHO IPC Consultant suspects, continued to preach the biased tenets of #DropletDogma via their interviews in this article.
What shocked me is the lack of scientific fact-checking from the so-called "Science Editor" @sarahknapton.
2/
What shocked me is the lack of scientific fact-checking from the so-called "Science Editor" @sarahknapton.
2/
Two egregious things stick out, which amount to journalistic malpractice.
1) Citing the interviewees biased, failed review as evidence that Airborne Transmission isn't occurring
2) Referencing year-old, obsolete comments from Dr. Klompas, without mentioning his recent work
3/
1) Citing the interviewees biased, failed review as evidence that Airborne Transmission isn't occurring
2) Referencing year-old, obsolete comments from Dr. Klompas, without mentioning his recent work
3/




1) The article references this WHO-funded, biased, "systematic review" preprint, which FAILED Peer Review and has been universally panned by respected peers in the field. Read the Peer Review AND the Comments. This Review has yet to be published.
f1000research.com/articles/10-23…
4/
f1000research.com/articles/10-23…
4/

Heneghan's claim (made in the article and the review) that "no study has found viable viral particles in the air that could have gone on to infect someone", is a lie.
Lednicky has successfully cultured virus from air twice. Dr. Tellier/Dr. Tang pick a part the criticisms here:
5/
Lednicky has successfully cultured virus from air twice. Dr. Tellier/Dr. Tang pick a part the criticisms here:
5/

Also recall that @trishgreenhalgh et al's widely lauded Lancet paper, was a direct response to this biased "Systematic Review".
It seems Heneghan and co. couldn't get their paper published and past a peer-review, so they went to the @Telegraph.
6/
thelancet.com/article/S0140-…
It seems Heneghan and co. couldn't get their paper published and past a peer-review, so they went to the @Telegraph.
6/
thelancet.com/article/S0140-…
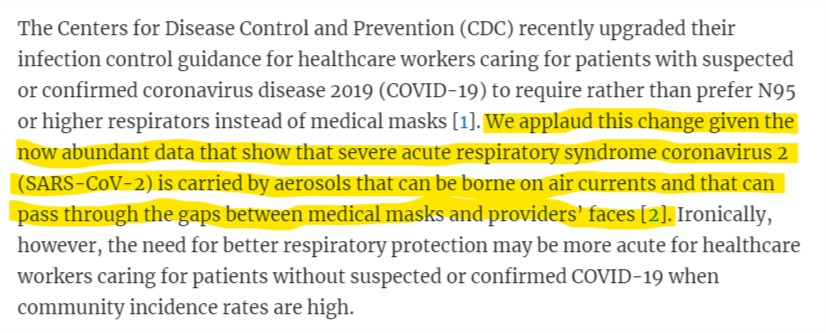
The second point, which I found to be most egregious, was the way @sarahknapton selectively used a year-old quote from Dr. Michael Klompas (ID MD from Harvard), without disclosing that Klompas has spent the past year publishing papers in support of Aerosol Transmission.
7/
7/
Here's one recent paper, where Klompas explicitly acknowledges aerosol and airborne transmission, and argues for universal N95 use (Airborne Precautions) when community transmission is high, instead of Surgical masks (Droplet Precautions).
8/
https://twitter.com/AbraarKaran/status/1403430911719268353?s=20
8/
Here's another recent study that Klompas was an author on, looking at nosocomial transmission in hospitals, despite social distancing and closed curtains, and in absence of Aerosol Generating Procedures.
9/
https://twitter.com/AbraarKaran/status/1406295871587713032?s=20
9/

And we can't forget this critical Klompas study, which proved nosocomial transmission despite Droplet Precautions, and makes a strong argument for more wide-spread N95 use (ie. Airborne Precautions).
academic.oup.com/cid/advance-ar…
10/
academic.oup.com/cid/advance-ar…
10/

So to frame Dr. Klompas, as an ID expert that is opposed to Aerosol Transmission in August 2021, is frankly egregious. If the @Telegraph and @sarahknapton want to have even a shred of credibility going forward, they should probably update this article.
11/
11/
To close, I'll link to a summary of studies providing evidence for Airborne Transmission. Decide for yourself if they're "low quality".
The vast majority PASSED peer-review and were published in prestigious journals.
Something that cannot be said about the Heneghan Review.
12/
The vast majority PASSED peer-review and were published in prestigious journals.
Something that cannot be said about the Heneghan Review.
12/




Final tweet with the last 2 pages of studies. And this list doesn't even scratch the surface of available evidence.
Key takeaways:
#COVIDisAirborne
#ReleaseTheN95s
#UpgradeYourMask
#ventilation
#filtration
#ReleaseTheEngineers
end\
Key takeaways:
#COVIDisAirborne
#ReleaseTheN95s
#UpgradeYourMask
#ventilation
#filtration
#ReleaseTheEngineers
end\



• • •
Missing some Tweet in this thread? You can try to
force a refresh










