The Pfizer booster trial is pretty spectacular.
10k previously 2x dosed (median 11 months from dose 2).
Randomised 1:1 placebo and 30ug.
95.6% relative risk reduction in symptomatic infection in intervention arm vs control (2dose only).
5 v 109 events 7+ days from boost.
10k previously 2x dosed (median 11 months from dose 2).
Randomised 1:1 placebo and 30ug.
95.6% relative risk reduction in symptomatic infection in intervention arm vs control (2dose only).
5 v 109 events 7+ days from boost.
To repeat: 95.6% RR reduction in symptomatic infection was for 3 vs 2 DOSES
UK data has 2dose Pfizer at ~80% VE vs symptomatic infection in Delta era. But follow up time <11 months in Pfizer trial.
If boost anywhere near 90% RR⬇️ we're looking at ~98% VE vs immunonaive.
UK data has 2dose Pfizer at ~80% VE vs symptomatic infection in Delta era. But follow up time <11 months in Pfizer trial.
If boost anywhere near 90% RR⬇️ we're looking at ~98% VE vs immunonaive.
They found no statistical difference for age, sex, race, ethnicity, or co-morbidities within the limitation of study size.
The primary course in the trial would have been with a 3-4 week dose interval between dose1 and dose2. (cf 10 week typical in UK).
pfizer.com/news/press-rel…
The primary course in the trial would have been with a 3-4 week dose interval between dose1 and dose2. (cf 10 week typical in UK).
pfizer.com/news/press-rel…
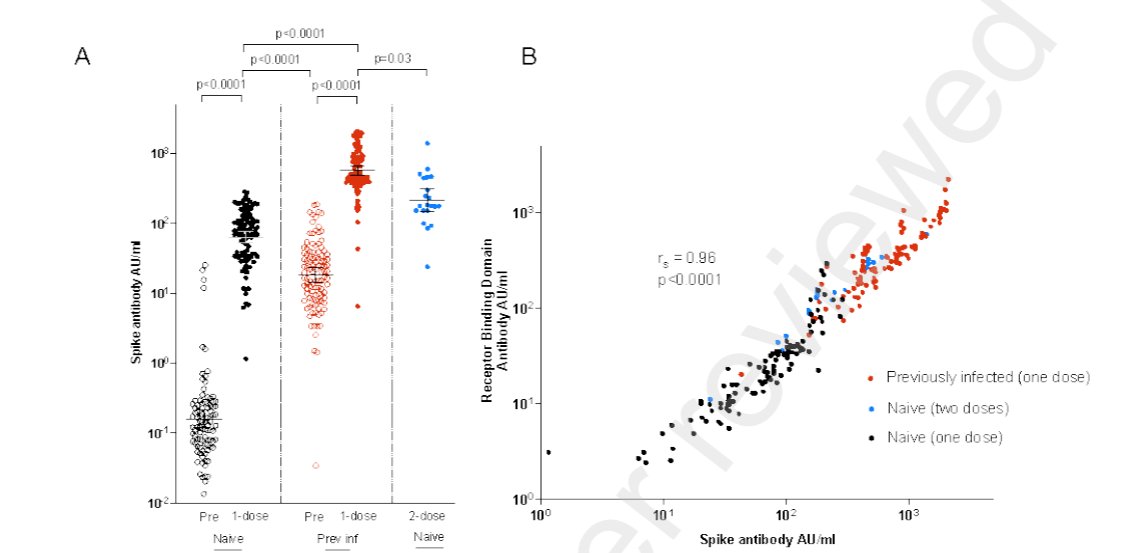
Phase2 neutralisation data that complements this RCT👇
We should just call Pfizer a 3 dose primary vaccine regimen (others similarly).
We should just call Pfizer a 3 dose primary vaccine regimen (others similarly).
https://twitter.com/asherichia/status/1451108228721414144
• • •
Missing some Tweet in this thread? You can try to
force a refresh