1/12 The cognitive load on rounds can be high, so I like using daily e-mails as an adjunct to teaching on rounds. Here is a 🧵 on my approach! #MedTwitter #MedEd #FOAMEd
2/ I am of the opinion that you can form an outline of a lesson plan BEFORE you even start on service! My group attends for 14 days at a time, so this tells me how much “time” I have allotted to teach (more on this later).
3/ Make sure to include every learner who will rotate with you while you are on (I use amion to figure out which trainees are on with me). They might appreciate getting learning when they are off service and if there is an ongoing thread of teaching, they won’t miss out!
4/ Next, we have to figure out what we are going to teach!Check out my thread here on some resources that I have aggregated.
Understanding your learner’s preferred modality is CRITICAL.
https://twitter.com/SatyaPatelMD/status/1453481988191518724?s=20.
Understanding your learner’s preferred modality is CRITICAL.
5/ Once you have decided on the material that you are going to teach, you can decide when you are going to deliver it (I decide on the day prior whenever possible). 

6/ I only give 3 teaching points per day plus an extra. I break it down into two buckets
1⃣Learning points
2⃣Spaced repetition
The spaced repetition only occurs AFTER day 2 (more on this later).
1⃣Learning points
2⃣Spaced repetition
The spaced repetition only occurs AFTER day 2 (more on this later).
7/ I then divide the points into subtypes (catered to my learner's learning preferences/needs). This allows me to highlight the learning that can occur on patients who are perceived to not be “medically active.” I do not use all subtypes every time!

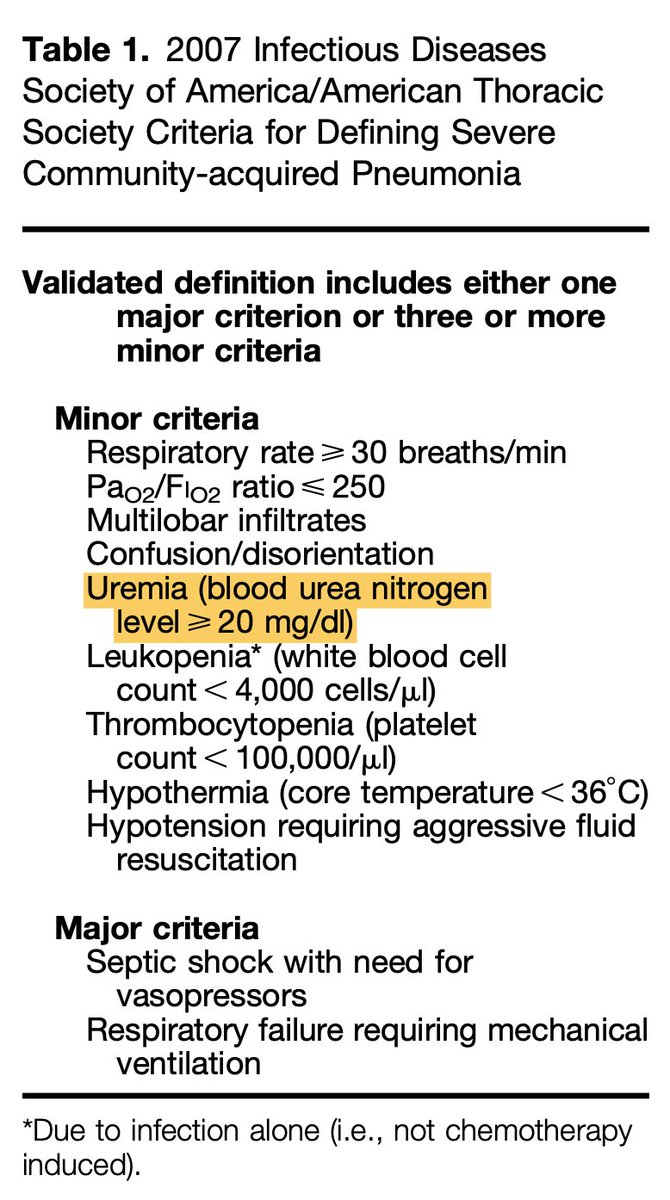
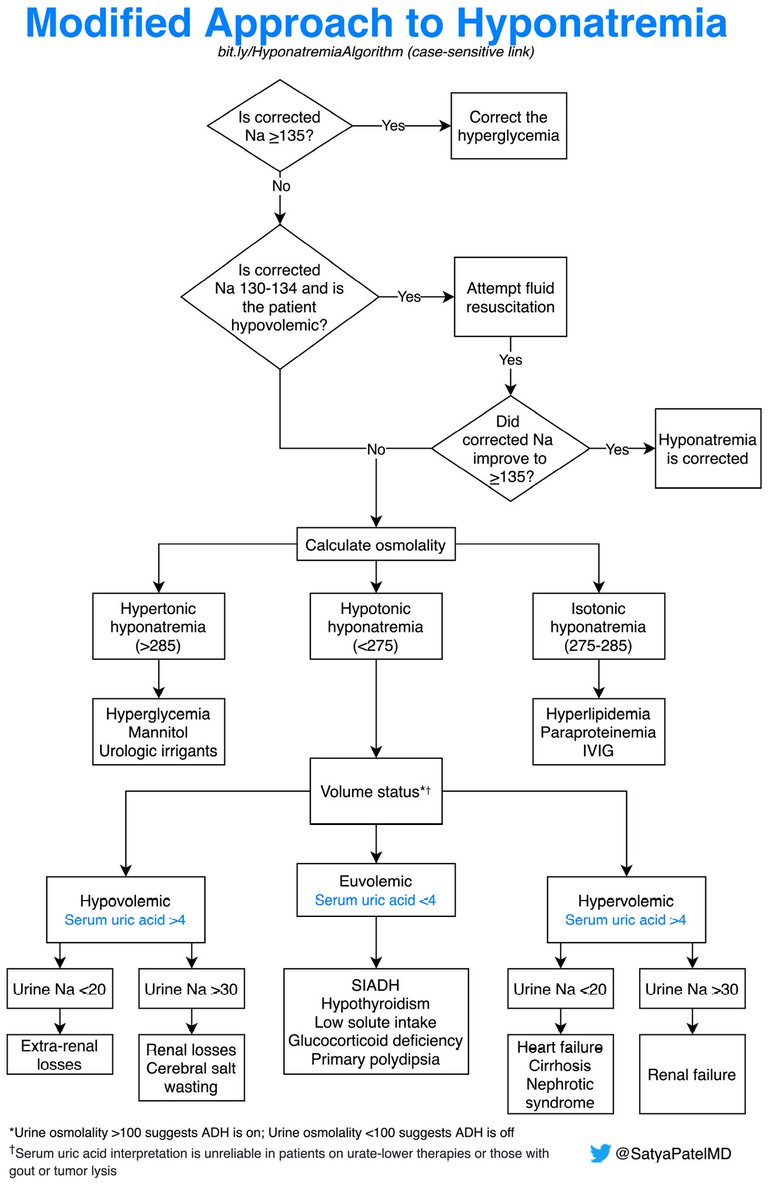
8/ Once I decide on the learning points, I then put the patient’s last name, the reason for admission, and then the pertinent finding related to the teaching point). This provides context to trainees that have since rotated off service. Try to include references!
9/ Back to your⏱️ on service. This is important because you can make a 14-point thread for teaching that you can discuss exclusively on e-mail. For instance, I am currently reviewing the incredible thread by @DrMarthaGulati on new chest pain guidelines:
https://twitter.com/DrMarthaGulati/status/1453785120780034048?s=20
10/ Starting on Day 3 I include spaced repetition, which is a copy-paste of prior learning points. I strongly believe that clear explanation + consistent repetition leads to long-term retention.
11/ You may think, “wow, this is a ton of work!” I agree that it is in the beginning, but so many points repeat themselves, so make sure to make the subject line of the e-mail consistent, that way you can easily search for prior emails with learning points.
12/12 In summary
✴️Include learners for your entire time on service
✴️Limit learning points to 3 and subdivide when appropriate
✴️Consider longitudinal teaching exclusively on e-mail
✴️Include spaced repetition
I would love to hear what others do!
✴️Include learners for your entire time on service
✴️Limit learning points to 3 and subdivide when appropriate
✴️Consider longitudinal teaching exclusively on e-mail
✴️Include spaced repetition
I would love to hear what others do!
• • •
Missing some Tweet in this thread? You can try to
force a refresh