Yesterday @SSI_dk released a forecast for omicron's spread in Denmark: ssi.dk/-/media/cdn/fi…
The forecast should be of wide interest as DK is intensively testing & sequencing. The situation is likely not worse here than elsewhere. It is just known.
A 🧵 on this forecast (1/9)
The forecast should be of wide interest as DK is intensively testing & sequencing. The situation is likely not worse here than elsewhere. It is just known.
A 🧵 on this forecast (1/9)
Some key premises for the forecast:
- The forecast includes both delta and omicron
- Waning immunity is included. It is assumed that immunity is 0.70 against O relative to D and that immunity against O wanes faster
(2/9)
- The forecast includes both delta and omicron
- Waning immunity is included. It is assumed that immunity is 0.70 against O relative to D and that immunity against O wanes faster
(2/9)
More premises:
- DK is rapidly rolling out boosters to face O. 1/3 of all are boosted! This is included
- Not all restrictions are included, especially not closing of most cultural activities from today
- Includes people's voluntary behavior change as infections rise
(3/9)
- DK is rapidly rolling out boosters to face O. 1/3 of all are boosted! This is included
- Not all restrictions are included, especially not closing of most cultural activities from today
- Includes people's voluntary behavior change as infections rise
(3/9)
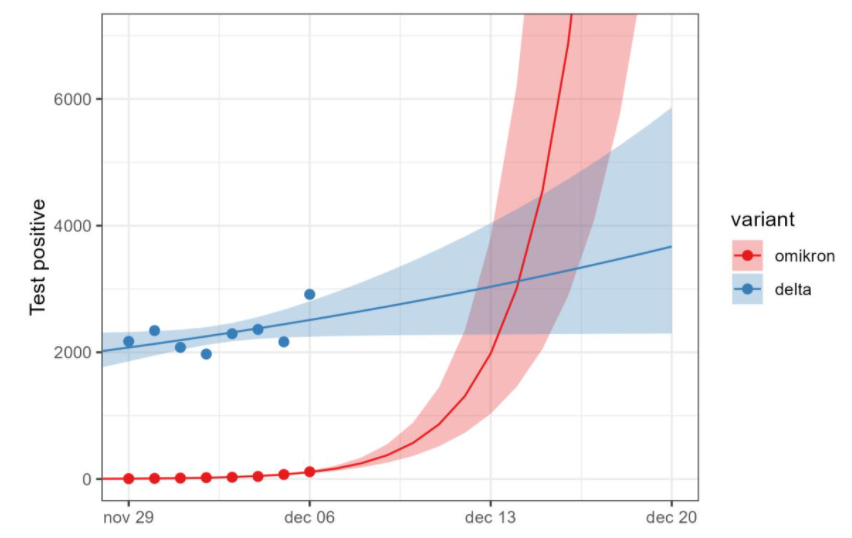
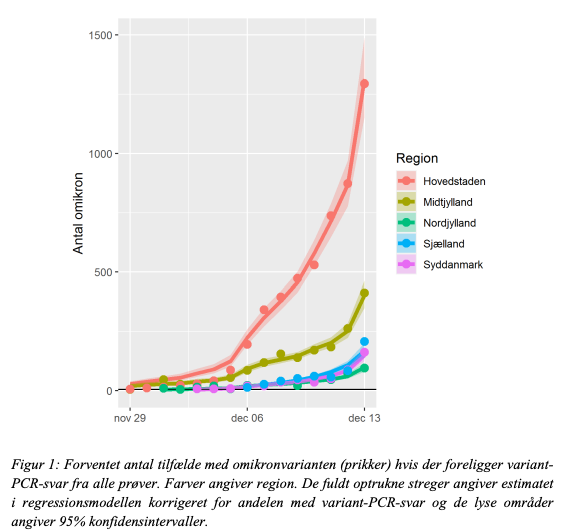
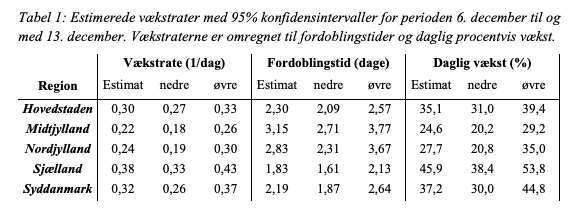
The models are based on this data from the spread of O in the five Danish regions. In the capital region ("Hovedstaden"), where most infections occur, O is to have a daily growth rate of .30, a doubling time of 2.3 days and a daily growth of 35 %. (4/9)
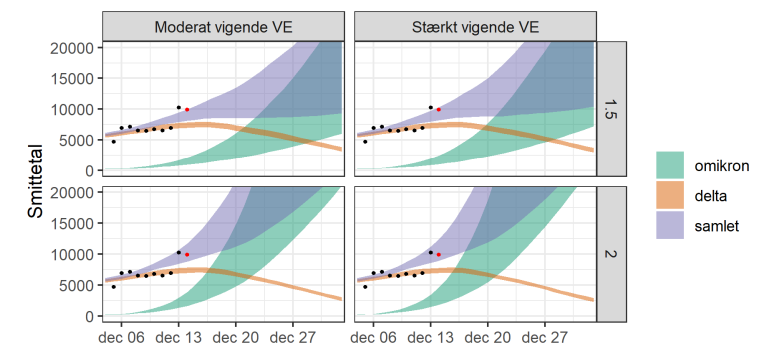
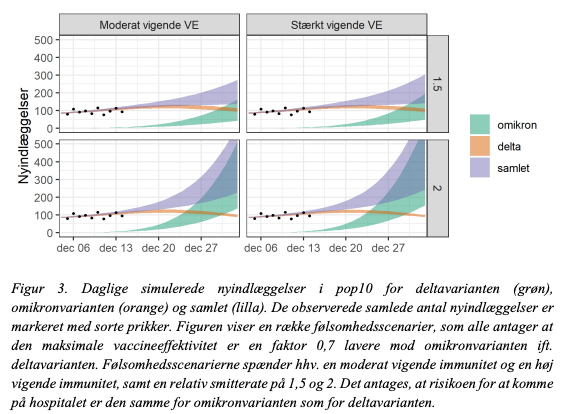
The core model is this showing the estimated cases over Xmas. The orange curve is D, the green is O and the purple is the combined. There are 2*2 scenarios: (a) how fast the immunity wanes for O relative to D and (b) whether O spreads 1.5 or 2 times as fast as D. (5/9)
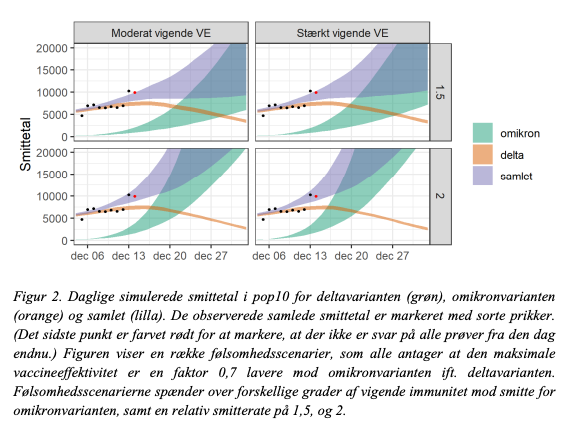
Depending on this, the models predicts from 9.000 to 45.000 cases. As we have already been above 9.000 this week, the lower-bound seems too low. (6/9)
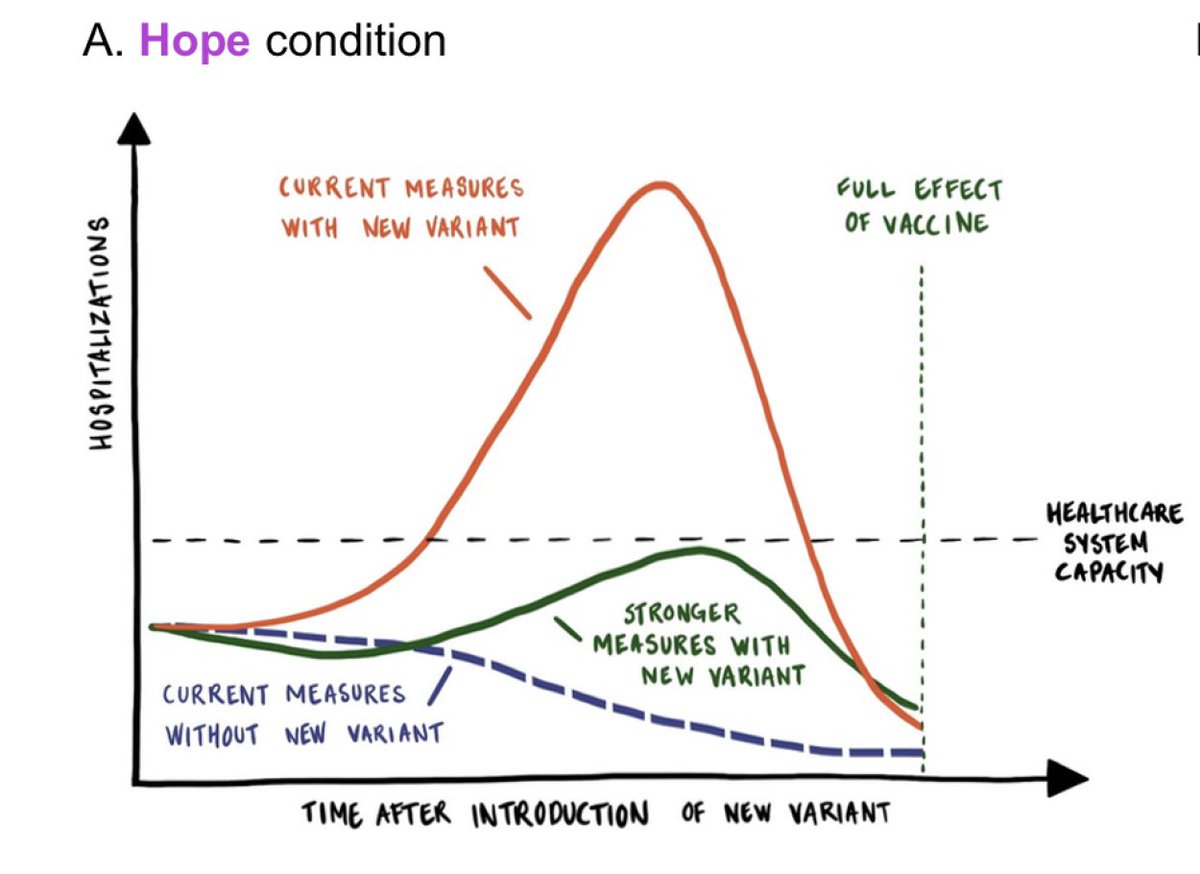
The key Q is how this translates into hospitalizations. This depends on the virulence of O. Fig 3 assumes similar virulence as D. Fig 4 assumes 50 % of the virulence of D. (7/9)
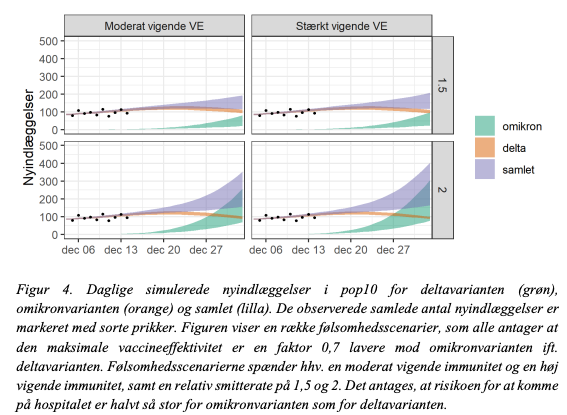
During our 2nd wave, daily hospitalizations were ~150 for ~3 weeks. The upper-bound of all models reach this but in the best case scenarios we will be able pull through with current interventions. The rapid roll-out of boosters is critical here. (8/9)
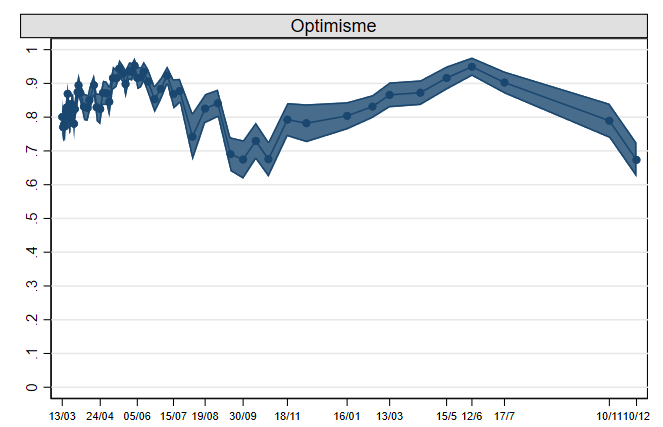
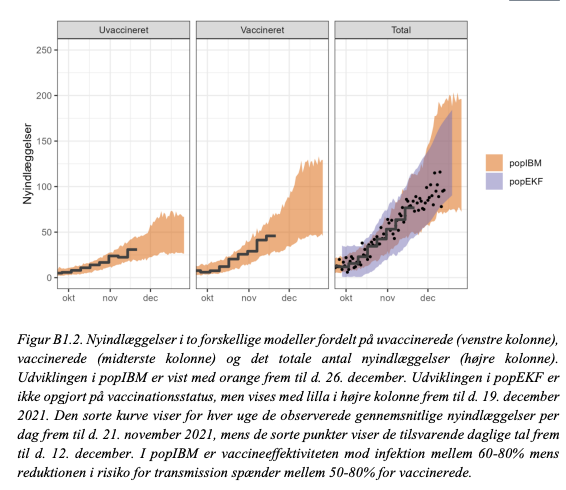
As the report notes there are many caveats and uncertainties. But overall the models in the report have been good at forecasting infection growth over the fall, as this fig shows. Of course, the uncertainties related to the transmission & virulence of O may change that. (9/9)
• • •
Missing some Tweet in this thread? You can try to
force a refresh