Electronic patient records (EPR) - I've seen some negative tweets recently about how cumbersome they can be...but EPR is here to stay so it's important to get them right
I'm fortunate to work somewhere with the most amazing EPR set-up...check it out!
A brief 🧵...
I'm fortunate to work somewhere with the most amazing EPR set-up...check it out!
A brief 🧵...
Our hospital's IT team have built 1 program from which we get all these options:
E-documents (clinic letters, memos etc)
Blood results
X-rays / scans
Drug chart
Request tests (bloods, imaging, micro, everything)
Link to primary care records
Observations (for in-patients)
E-documents (clinic letters, memos etc)
Blood results
X-rays / scans
Drug chart
Request tests (bloods, imaging, micro, everything)
Link to primary care records
Observations (for in-patients)

There's so much more there too..."Outpatients" allows us to see what we have booked for upcoming clinics including procedural clinic lists like stress echo.
EDMS has the scanned records after hospital admissions
There's even a direct link to UpToDate!
EDMS has the scanned records after hospital admissions
There's even a direct link to UpToDate!

Clicking on e-documents brings up the various specialities that letters are categorised by...and if you click on one division like 'Medicine', you can see the breakdown...so you know instantly where to look to find the letters you need
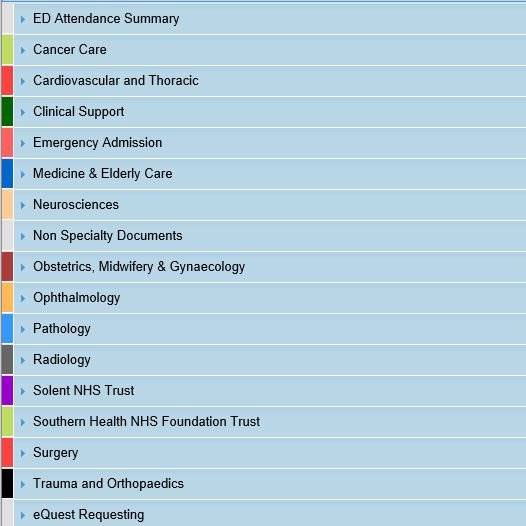

This is what the menu looks like...you can see if the document is a clinic letter, a MDT meeting entry, a record of a phone call with the patient, a GP referral, a test result (e.g. TTE or TOE) etc...so you can usually find what you want pretty quickly!

The eQuest system allows you to request almost any test, request a specialty consult from another team and also view requests already placed on the system, to avoid repetition / duplication

I know this is a rather unusual thread compared to my normal ones, but I see my wife struggle with her hospital's IT system - literally pulling her hair out at how clunky and difficult it is to navigate - and I realise that getting this right really impacts our working lives!
I've never met any of the @UHSDigital team, but a BIG thank-you from me (and I suspect almost everyone that works here) for a truly special IT system that definitely aids efficiency and facilitates patient care
Interested to hear experiences of others with EPR systems...
Interested to hear experiences of others with EPR systems...
• • •
Missing some Tweet in this thread? You can try to
force a refresh