Over 220 people attended this @CDCofBC Grand Round. Thank you to everyone who showed up, and for your pointed questions. 

Presentation was based on this study, not yet peer reviewed. Except perhaps on twitter by epidemiologists on twitter. @EpiEllie @FurnessColin @rdumont99 medrxiv.org/content/10.110…

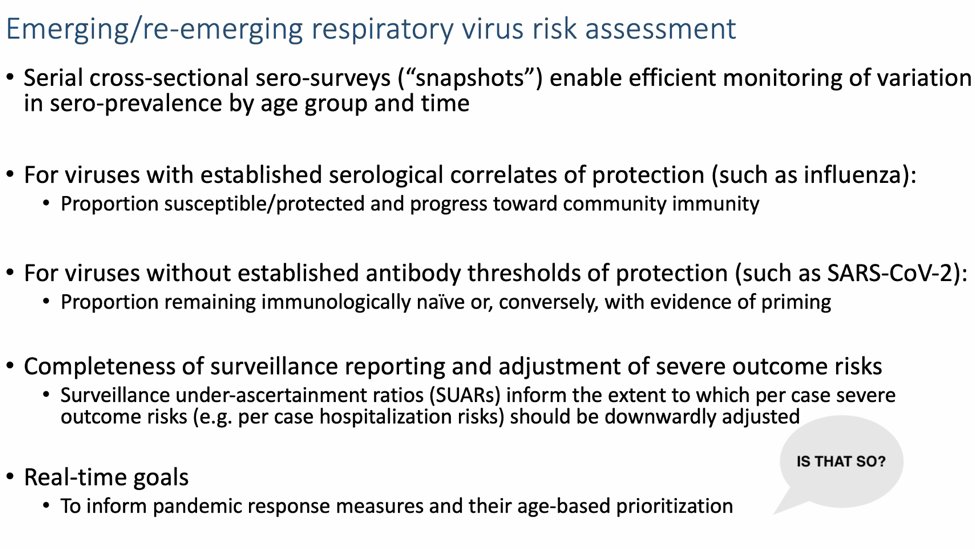
There were several obvious contradictions in the presentation. Expect a longer thread to follow. This below "real time goals" is likely the most egregious.
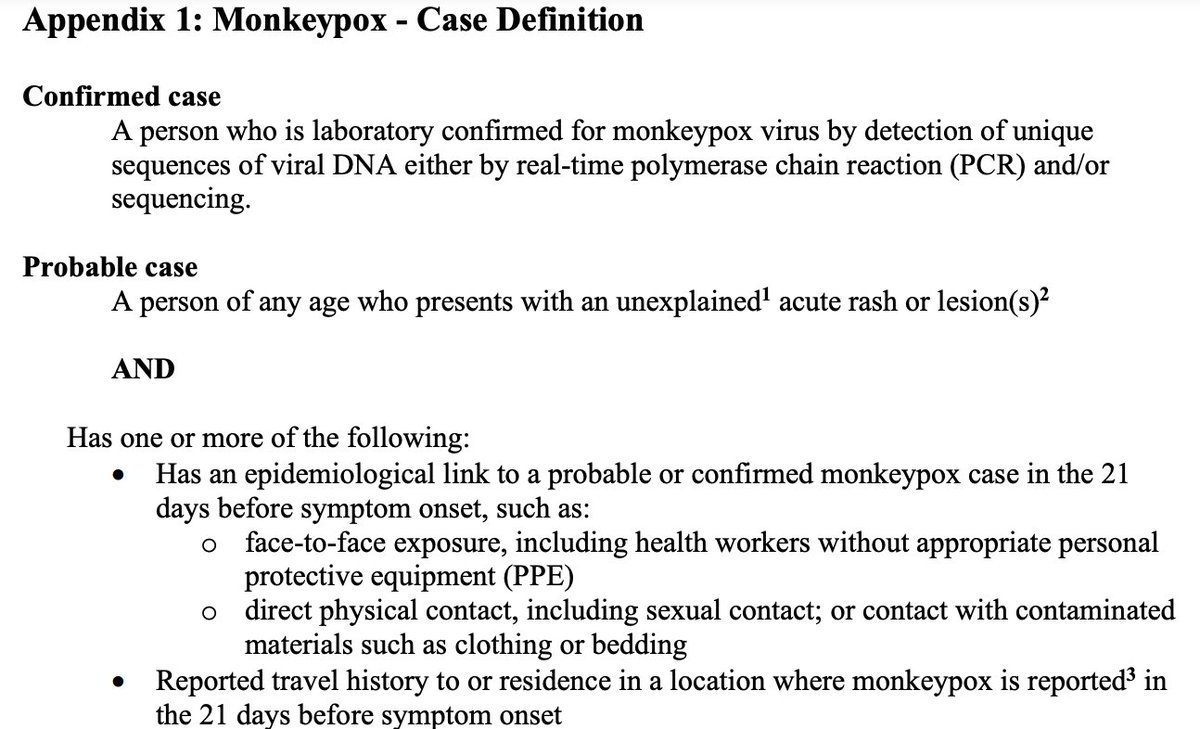
Source: @CDCofBC slide
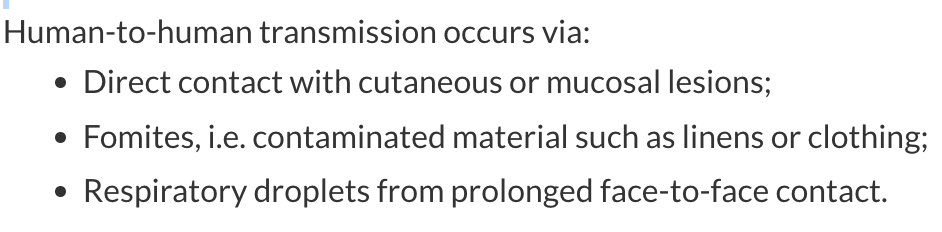
Source: @CDCofBC slide

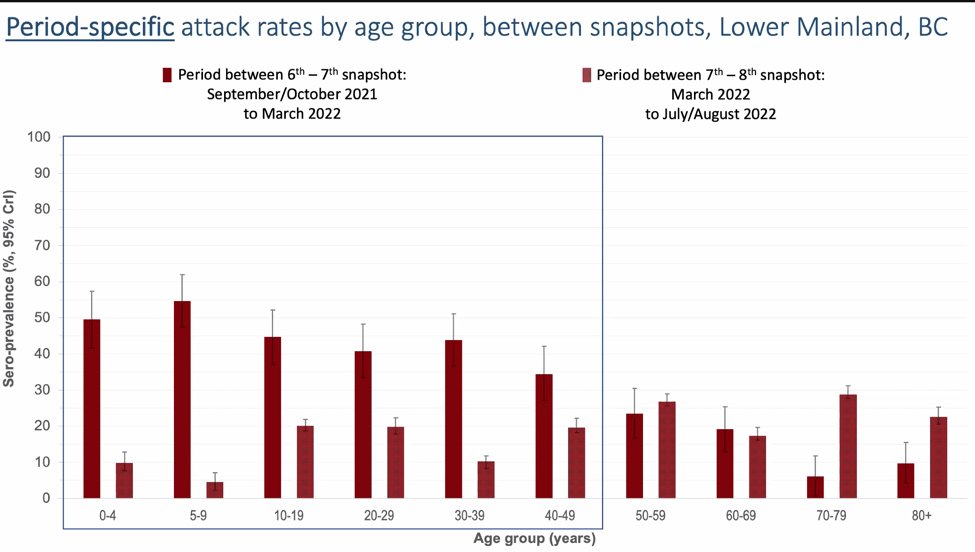
Another @CDCofBC slide, from Sept/Oct. 2021 to March 2022 , children were group most acutely infected with #COVID. % are in fact underestimation of real jump in VCH-FHA general community seroprevalence. Children attack rate > than parents age = School Transmission.
Presenter confirmed that data was presented to BC Public Health leaders. Seemed to be an emphasis on separation of roles: research vs policy making. Does not align with @CDCofBC website. Brits call this a "say-do gap." bccdc.ca/about/what-we-…
Also does not align with the stated real-time goals of the study.
A quote in the chat sums up the real ethical problem: "The study itself doesn't raise ethics concerns to me. What raises ethics concerns is the involvement of Dr. Bonnie Henry, particularly her being an author while simultaneously impacting the factors the study is examining..."
"- both the under-ascertainment / testing availability, and the measures / lack thereof that contributed to infection spread."
Expect authors to say they were not directly examining these factors. In fact, they were examining their outcomes: how many children were infected because inadequate protective measures were in place in schools. Meanwhile at pressers, parents/teachers heard schools were safe.
Data was there and yet no intervention happened to prevent further infections in children. Looks very much like Sweden, where leaders bought into "immunity through infection", especially infection of children. Heard word "silver lining" used in the BC CDC presentation.
PHO has denied infections occurred in schools.There has been no acknowledgement of the true study results by #bcpoli #bced Worse, still no interventions to make BC schools #Covid safe. Meanwhile, #Omicron infections and reinfections are happening.
• • •
Missing some Tweet in this thread? You can try to
force a refresh