NEXT Inventory and Comparison of ICU datasets by Christopher SAUER
"Why talk on differences in ICU databases?"
Ans: becuase data is "CORE"
@ESICM #ml #ai #databases #datascience #LIVES2022
"Why talk on differences in ICU databases?"
Ans: becuase data is "CORE"
@ESICM #ml #ai #databases #datascience #LIVES2022
@ESICM Merit of publicly available ICU databases
- no randomzined evidence exists for most clinical situations
-data and pt level insights incredibly useful.
-local epidemiology and treatment difers
-real world data sets help deliver optimal treatment policies.
#DataScience #LIVES2022
- no randomzined evidence exists for most clinical situations
-data and pt level insights incredibly useful.
-local epidemiology and treatment difers
-real world data sets help deliver optimal treatment policies.
#DataScience #LIVES2022
@ESICM 1st publicly available dataset MIMIC-3 in 2016,
Beth Israel Deaconess Medical Centre, Boston,MA
>70,000 icu stays, 2008 to 2019
now also includes chest x-rays, emergency room data
- large, community developed Github repo.
#DataScience
Beth Israel Deaconess Medical Centre, Boston,MA
>70,000 icu stays, 2008 to 2019
now also includes chest x-rays, emergency room data
- large, community developed Github repo.
#DataScience
@ESICM Systemetic review
1. what publicly availa data sets exist
2. what patient characteristics, admission population, treatment intensity, outcomes compare ?
3. which databases suited for which type of research
4. what consequences for transferability?
(excellent pertinent questions)
1. what publicly availa data sets exist
2. what patient characteristics, admission population, treatment intensity, outcomes compare ?
3. which databases suited for which type of research
4. what consequences for transferability?
(excellent pertinent questions)
@ESICM 4 publicly available datasets identified
1.Amsterdam UMCdb - 20k icu patients
2. eICU-CRD (collab with Philips)
3. HiRID
4. MIMIC
1.Amsterdam UMCdb - 20k icu patients
2. eICU-CRD (collab with Philips)
3. HiRID
4. MIMIC
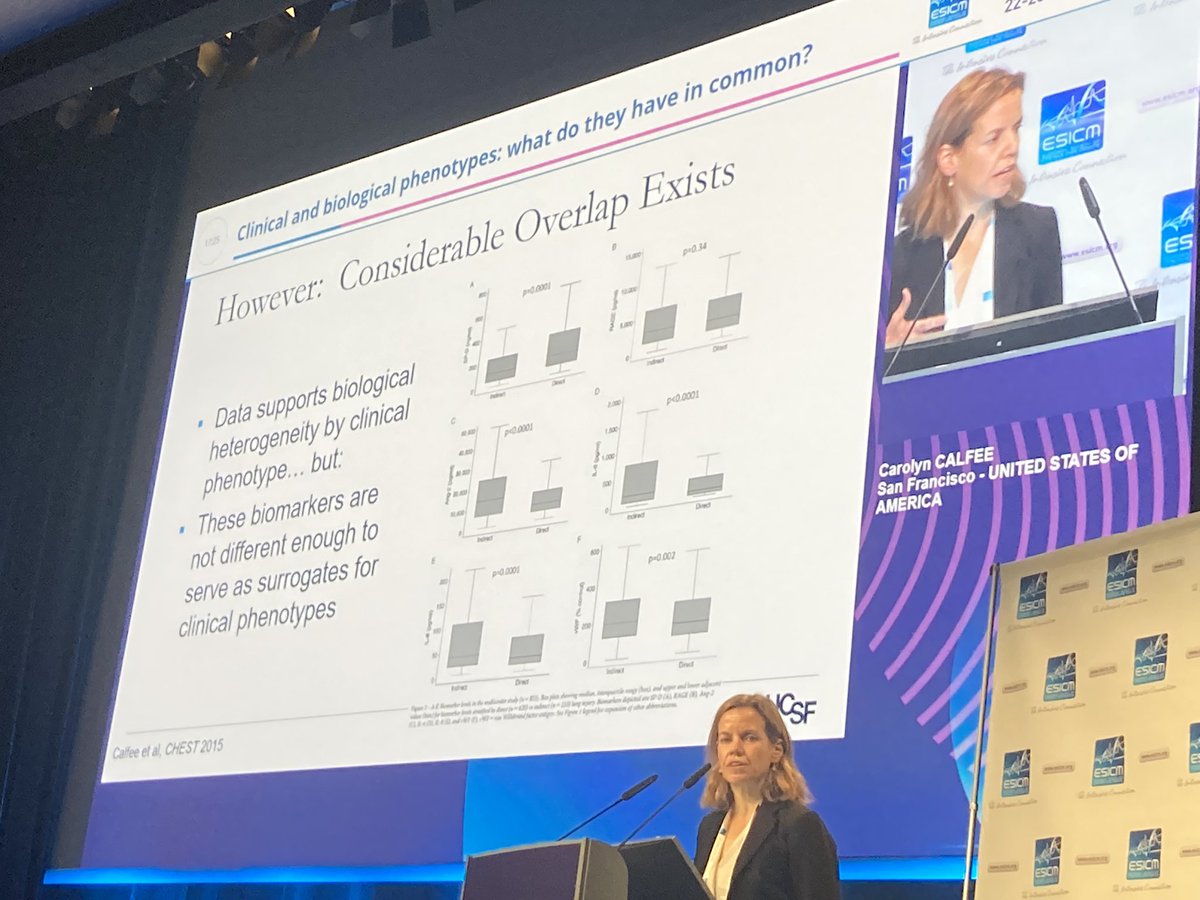
Differences in admission 

Have different frequencies. Have an issue if it’s time series modelling

Most eye opening for Sauer himself is different treatment intensity and outcomes.
- significantly upto x3 higher ICU mortality
vasopressor use 69% in Amsterdam vs eICU 12% and MIMIC 31%
-invasive ventilator use 83% in amsterdam vs 33 in MIMIC
- significantly upto x3 higher ICU mortality
vasopressor use 69% in Amsterdam vs eICU 12% and MIMIC 31%
-invasive ventilator use 83% in amsterdam vs 33 in MIMIC
-emergency admn icu mortality 18.3% vs. 8.9% in MIMIC IV
This is fascinating.
Perhaps admission thresholds different in public v private systems OR USA v. EU for example.
This is fascinating.
Perhaps admission thresholds different in public v private systems OR USA v. EU for example.
Individual strengths and weaknesses

Thus, findings may not be generalisable. Model re-training required.
findings should be validated in at least 2 data sets. models may require adjustments according to variable availability and distributions
findings should be validated in at least 2 data sets. models may require adjustments according to variable availability and distributions
Key take-away's
- "best" icu data set depends on research question
- be prepared to adjust your models
- hope that in next few years, there will be database from outside of Western Europe.@ESICM (interesting final point of equity of ML too) #datascience #criticalcare #ai
- "best" icu data set depends on research question
- be prepared to adjust your models
- hope that in next few years, there will be database from outside of Western Europe.@ESICM (interesting final point of equity of ML too) #datascience #criticalcare #ai
Author happy to be reached out. linkedin.com/in/cmsauer/
Q : what EHR vendor you have impacts on the database?
A : interesting question. doesnt know about vendor but potentially could have consequences. equally, people's attitude to privacy and how each health system stringently structures and saves their data makes a difference.
A : interesting question. doesnt know about vendor but potentially could have consequences. equally, people's attitude to privacy and how each health system stringently structures and saves their data makes a difference.
in summary, less of a vendor and more of how a health system uses that to collect,save and store the data likely to make a bigger difference.
• • •
Missing some Tweet in this thread? You can try to
force a refresh