MORE STINKY CHEESE 🧀🧀🧀
#thalidomideViki quotes the discredited @thelancet again, because it suits her agenda.
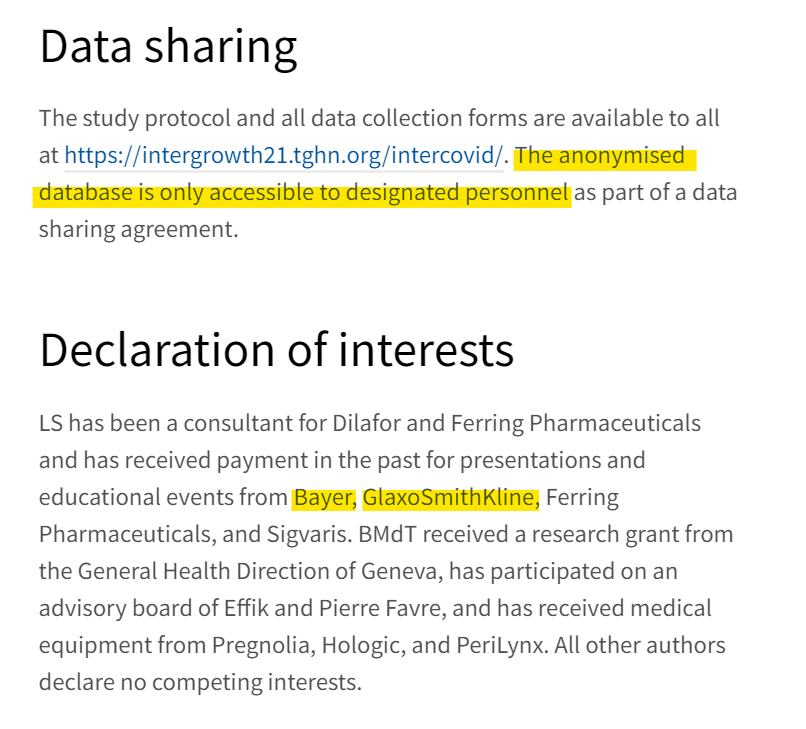
This study should be completely disregarded as real because data sharing is declined - again.
Every study Viki posts is not verifiable.
But there's more...
#thalidomideViki quotes the discredited @thelancet again, because it suits her agenda.
This study should be completely disregarded as real because data sharing is declined - again.
Every study Viki posts is not verifiable.
But there's more...
https://twitter.com/VikiLovesFACS/status/1615630315120205825
Immediate red flags are differences in the groups, such as the higher prevalence of smoking in the "COVID" group which hasn't been seen in real world studies. And the smoker group had the exact same educational history - you don't usually see that.


Always worth looking at the supplementary to look for inconsistencies in published data.
These figures on a test negative design show that the "effectiveness" was only 9%. Bearing in mind miscategorisation bias, this means there was negative efficacy against infection.
These figures on a test negative design show that the "effectiveness" was only 9%. Bearing in mind miscategorisation bias, this means there was negative efficacy against infection.



And, as we have seen previously, these non-randomised studies bias towards smokers in the unvaccinated group, which is the primary driver for preterm labour.
Oh look (RR=0.78, p<0.05)
Oh look (RR=0.78, p<0.05)

Table 3b gives the outcomes for those pesky "unvaccinated" women by COVID status, showing the only fetal outcome difference was preterm birth, which could entirely be accounted for by the group smoking rates.
This is a sham.
This is a sham.

Remember @thelancet via @richardhorton1 published the laughable #surgisphere fraud for which they have never apologised.
They just keep churning out unverifiable pro-pharma drivel, never allowing the data to be independently verified.
They just keep churning out unverifiable pro-pharma drivel, never allowing the data to be independently verified.
https://twitter.com/JikkyKjj/status/1479634865129590785
And now the paper turns quite dark.
The UK maternal mortality rate is 7 per 100,000 births (2017).
In this series of unvaccinated women there were 4 deaths. This should not have happened. The probability of 4 deaths in 1732 patients... 0.00001
The UK maternal mortality rate is 7 per 100,000 births (2017).
In this series of unvaccinated women there were 4 deaths. This should not have happened. The probability of 4 deaths in 1732 patients... 0.00001

Note that the table 3b breakdown was not published for the vaccinated women, demonstrating an innate bias by the authors.
And one death has been removed in table 5, which should have 5 deaths in total if there was one death in the vaccinated group.
And one death has been removed in table 5, which should have 5 deaths in total if there was one death in the vaccinated group.

If there truly were 4 or 5 deaths in this series of 2738 pregnant women, the whole trial group should must be audited because this level of maternal mortality is off the scale.
Of course #thalidomideViki and #ACIPKevin wouldn't be interested in any of this...
Of course #thalidomideViki and #ACIPKevin wouldn't be interested in any of this...
Because they don't read the supplementaries and they don't understand the limitations of the data and they don't understand clinical trials.
They also don't understand that when 50+ authors "write" a paper 49+ of them had no input into the calculations or validation.
They also don't understand that when 50+ authors "write" a paper 49+ of them had no input into the calculations or validation.
So I am going to charge @thelancet to prove that this paper was not ghost-written and to release the full anonymised data set - or retract the paper.
And one last thing...
@franklin_reeder @Double_Christ @TonyNikolic10
And one last thing...
@franklin_reeder @Double_Christ @TonyNikolic10
Those 5 deaths... 4 were in the unvaccinated who received antibiotic treatment at a lower rate despite having "more COVID". Which likely means they had treatment withheld compared to the vaccinated group.
If that was the #3tablets needed for post-viral pneumonia...
If that was the #3tablets needed for post-viral pneumonia...
It would suggest that those women were treated with prejudice, which resulted in their death.
So I am calling on EVERY death in that paper to be criminally and independently investigated.
Because it's happening.
Don't believe me? Read this:
thewayout.substack.com/p/the-war-on-l…
So I am calling on EVERY death in that paper to be criminally and independently investigated.
Because it's happening.
Don't believe me? Read this:
thewayout.substack.com/p/the-war-on-l…
• • •
Missing some Tweet in this thread? You can try to
force a refresh