A 14-yo ♂️ lived on a farm: a 1-month history of episodic headaches, vomiting, & papilledema
MR: a multiloculated cyst of the brain (A) with a hypointense rim and small projections in T2 phase (B, arrow)
1/5
DOI: 10.1056/NEJMicm2208104
#neurology #radiology #pediatric
MR: a multiloculated cyst of the brain (A) with a hypointense rim and small projections in T2 phase (B, arrow)
1/5
DOI: 10.1056/NEJMicm2208104
#neurology #radiology #pediatric
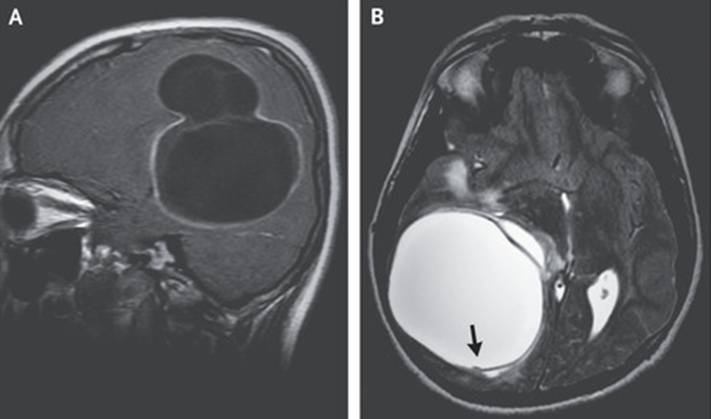
Findings suggestive of CYSTIC ECHINOCOCCOSIS.
CT of the body: no other sites of disease.
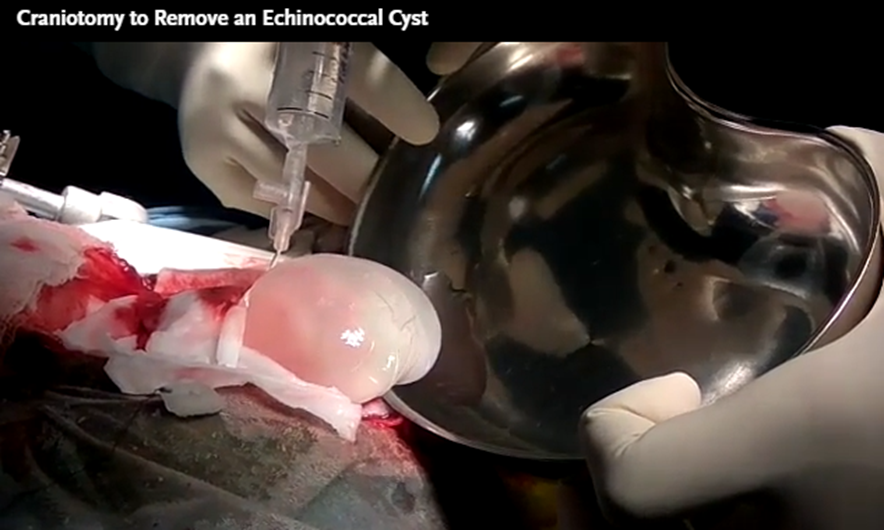
A craniotomy was performed, during which saline irrigation was used to separate the cyst wall from the brain to avoid rupture.
2/5
DOI: 10.1056/NEJMicm2208104
#IDtwitter #parasitology
CT of the body: no other sites of disease.
A craniotomy was performed, during which saline irrigation was used to separate the cyst wall from the brain to avoid rupture.
2/5
DOI: 10.1056/NEJMicm2208104
#IDtwitter #parasitology
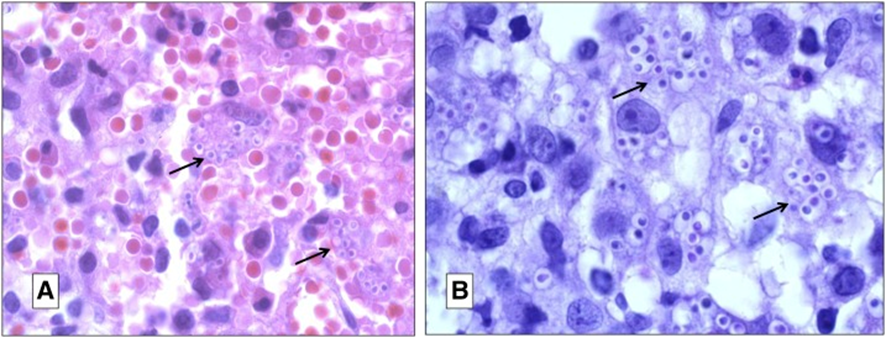
🔬: an echinococcal laminated membrane lined by a germinal layer with daughter cysts (Panel D, arrows) and protoscolices (inset, arrows) with hooklets (arrowhead).
PRIMARY CEREBRAL CYSTIC ECHINOCOCCOSIS FROM ECHINOCOCCUS GRANULOSUS
3/5
#microbiology #Pathologists #pathology
PRIMARY CEREBRAL CYSTIC ECHINOCOCCOSIS FROM ECHINOCOCCUS GRANULOSUS
3/5
#microbiology #Pathologists #pathology

A 3-month course of albendazole was prescribed
At the 2-week follow-up, the patient’s symptoms had resolved.
4/5
#MedTwitter #Doctor
At the 2-week follow-up, the patient’s symptoms had resolved.
4/5
#MedTwitter #Doctor
Echinococcal cysts (hydatid cysts) most commonly form in the liver.
The infection is transmitted through contact with infected livestock or canine feces, as was likely to have happened in this case.
5/5
#MedStudentTwitter #resident #medicine
The infection is transmitted through contact with infected livestock or canine feces, as was likely to have happened in this case.
5/5
#MedStudentTwitter #resident #medicine

• • •
Missing some Tweet in this thread? You can try to
force a refresh