
1/ #Metabolism, #lipids, and #ASCVD
#megathread🧵🧵🧵
Okay, I want to revisit and breakdown my position on this crucial topic and the challenges in communicating it.
⚠️ Get comfortable, as this could get long.
Ready? Let's go...
#megathread🧵🧵🧵
Okay, I want to revisit and breakdown my position on this crucial topic and the challenges in communicating it.
⚠️ Get comfortable, as this could get long.
Ready? Let's go...
https://twitter.com/theproof/status/1638656893785878528

2/ First, it's worth reviewing why there's a high level of confidence low density lipoproteins (LDLs) drive atherosclerotic cardiovascular disease (ASCVD)
For an excellent, lay-person video, I recommend @NutritionMadeS3's from a couple years ago 👇
For an excellent, lay-person video, I recommend @NutritionMadeS3's from a couple years ago 👇
https://twitter.com/realDaveFeldman/status/1375628657629097987?s=20
3/ Also in the name of arguably the most cited meta-analysis for the Lipid Hypothesis to date:
"Low-density Lipoproteins cause atherosclerotic cardiovascular disease"
This meta combines lines from genetic, observational, and interventional studies.
pubmed.ncbi.nlm.nih.gov/28444290/
"Low-density Lipoproteins cause atherosclerotic cardiovascular disease"
This meta combines lines from genetic, observational, and interventional studies.
pubmed.ncbi.nlm.nih.gov/28444290/
4/ Now if you've followed me through the years, you know I regularly and often emphasize that...
... It's possible:
1) Lipid Hypothesis could be completely correct.
... and ...
2) #LowCarb diets with high LDL could be dangerous
Hence freq reminders 👇
... It's possible:
1) Lipid Hypothesis could be completely correct.
... and ...
2) #LowCarb diets with high LDL could be dangerous
Hence freq reminders 👇
https://twitter.com/realDaveFeldman/status/1474157060186992652?s=20
5/ So everything I discuss next is strictly under the umbrella of a hypothesis and shouldn't be taken as medical advice in any way. Sound good?
Okay – let's talk about ***Metabolism***
I know, I know, you hear the term all day long on #NutritionTwitter. But what is it, really?
Okay – let's talk about ***Metabolism***
I know, I know, you hear the term all day long on #NutritionTwitter. But what is it, really?
6/ For a simple answer, metabolism is the balance ⚖️ between...
🧱 "anabolism" (the building up of things) and
💥"catabolism" (the breaking down of things)
And the "things" we're especially interested in is protein and energy (fat and carbs)
🧱 "anabolism" (the building up of things) and
💥"catabolism" (the breaking down of things)
And the "things" we're especially interested in is protein and energy (fat and carbs)
7/ But I should expand on this a tiny bit more.
Metabolism isn't just the balance between these two modes, it's how good a body is at doing each of them...
... particularly with fuel. ⛽️⛽️⛽️
How good you are at putting fuel away and getting it back out again is very important
Metabolism isn't just the balance between these two modes, it's how good a body is at doing each of them...
... particularly with fuel. ⛽️⛽️⛽️
How good you are at putting fuel away and getting it back out again is very important
8/ So what does this have to do with lipids, particularly LDL?
Quite a lot, actually. Bear with me...
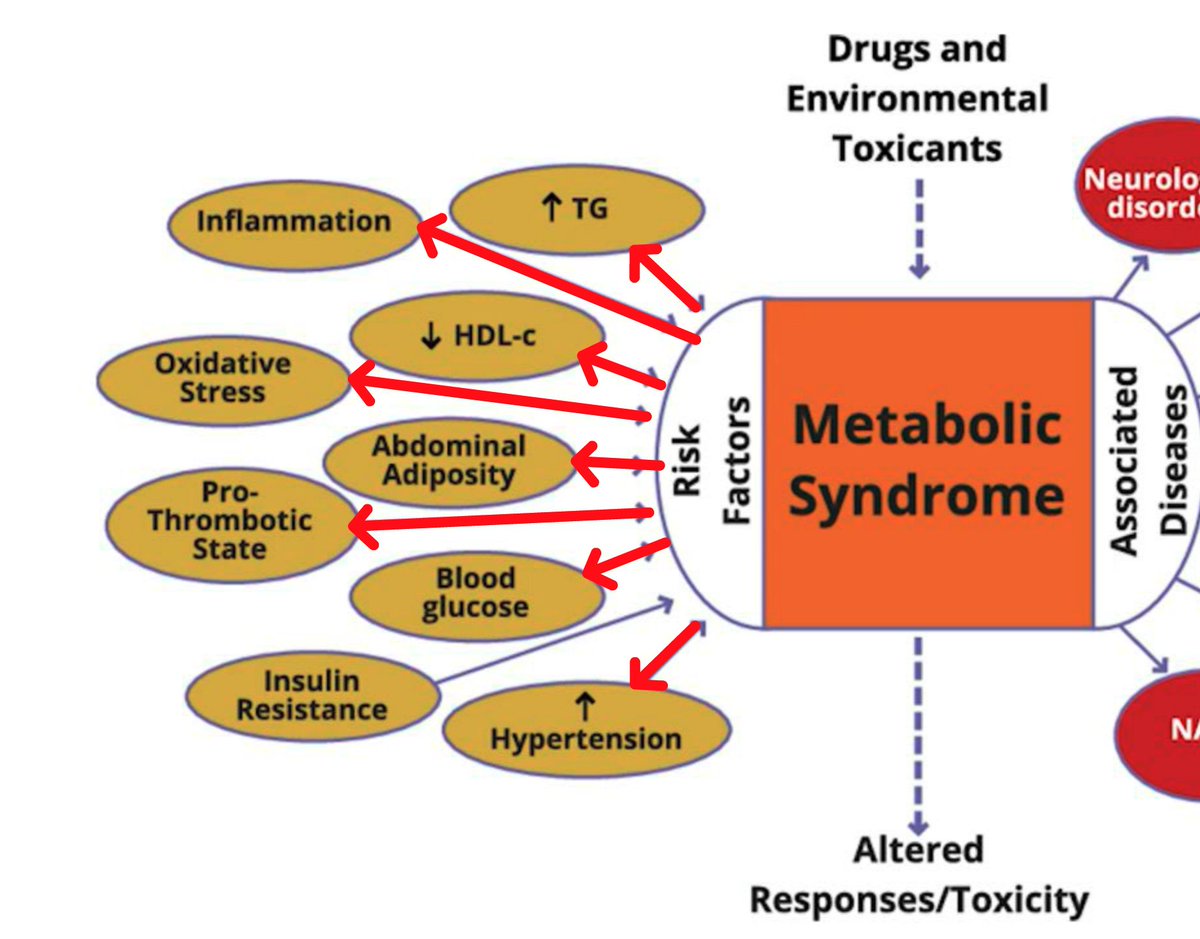
I'd like to pull out a great graphic from @theproof's recent podcast that combines a number of "risk factors" (left), "Metabolic Syndrome", and "Associated Disease" (right).
Quite a lot, actually. Bear with me...
I'd like to pull out a great graphic from @theproof's recent podcast that combines a number of "risk factors" (left), "Metabolic Syndrome", and "Associated Disease" (right).

9/ Okay... for those who don't know, what the heck is "Metabolic Syndrome"?
For this, I'll just post #ChatGPT's reply. 👇
But in short, it's at least 3 of the following:
-Abdominal obesity
-high glucose
-high blood pressure
-high triglycerides (TG)
-low HDL cholesterol (HDL)
For this, I'll just post #ChatGPT's reply. 👇
But in short, it's at least 3 of the following:
-Abdominal obesity
-high glucose
-high blood pressure
-high triglycerides (TG)
-low HDL cholesterol (HDL)

10/ Now hold it! 🛑 See those 5 criteria above?...
I've changed them. All of them. Plenty of times.
For example, 5 years ago I did the "White Bread and Processed Meat Experiment" (cholesterolcode.com/the-tandem-dro…)
In 7 days my:
HDL-C changed 55 ➡️ 38
and TG change 78 ➡️ 221
I've changed them. All of them. Plenty of times.
For example, 5 years ago I did the "White Bread and Processed Meat Experiment" (cholesterolcode.com/the-tandem-dro…)
In 7 days my:
HDL-C changed 55 ➡️ 38
and TG change 78 ➡️ 221
11/ Let me restate this for emphasis...
A 31% (!) HDL drop from 55 to 38 mg/dL meets one of the criteria for Metabolic Syndrome
A rise of 183%(!) for triglycerides likewise meets another.
But this is just some wonky, acute exercise, right?
A 31% (!) HDL drop from 55 to 38 mg/dL meets one of the criteria for Metabolic Syndrome
A rise of 183%(!) for triglycerides likewise meets another.
But this is just some wonky, acute exercise, right?

12/ Sure -- let's assume it is just a short term experiment and that my numbers will return in a matter of days to where they were on #keto.
That's not a reason to ignore this data, it's the exact opposite!
We need to look to short and long term metabolic influence on lipids...
That's not a reason to ignore this data, it's the exact opposite!
We need to look to short and long term metabolic influence on lipids...
13/ I'm demonstrating a state associated with chronic disease
***without the actual chronic disease***.
I'm intentionally inducing a state of elevated insulin (through constant consumption of white bread) resulting in many of the downstream characteristics of Metabolic Syndrome
***without the actual chronic disease***.
I'm intentionally inducing a state of elevated insulin (through constant consumption of white bread) resulting in many of the downstream characteristics of Metabolic Syndrome
14/ So returning to that graph, we understandably should ask -- how much of these risk factors are causing Metabolic Syndrome...
... vs Metabolic Syndrome causing these risk factors?
... vs Metabolic Syndrome causing these risk factors?
15/ Importantly, the more severe one's Metabolic Syndrome, the more they will also have:
Higher oxLDL
Higher "small dense" LDL
Less "big fluffy" LDL
@theproof -- with these too 👆 I strongly posit atherogenicity is less about independent causality than a reflection of the status
Higher oxLDL
Higher "small dense" LDL
Less "big fluffy" LDL
@theproof -- with these too 👆 I strongly posit atherogenicity is less about independent causality than a reflection of the status
16/ I appreciate that there's now more focus on the actual composition of the lipoproteins themselves, such as the level of triglyceride (TG) on LDLs.
The cargo on LDLs is like a manifest. It can help tell the story about what happened to the vehicle in its preceding stages.
The cargo on LDLs is like a manifest. It can help tell the story about what happened to the vehicle in its preceding stages.
17/ 🤓🤓🤓 [[[GEEK ASIDE: and for more detail on this, check out the interplay between CETP and lipoprotein lipase in their ultimate downstream effect on LDL composition. I'll again predict that same sized LDL between MetS vs LMHRs will have very different TG-CE composition]]]
18/ I realize there's enormous confidence that these various markers can be looked at in isolation and quantified for their independent contribution (or lack of) to plaque development (particularly ApoB).
I don't share that level of confidence, and posit metabolism is relevant.
I don't share that level of confidence, and posit metabolism is relevant.
19/ But until recently, there was no realistic scenario where we could get folks without some form of dysfunction in lipid metabolism (either via genetics, like monogenetic FH or acquired like MetS) with high LDL but low CVD risk factors otherwise.
Until #LMHRs, ofc...
Until #LMHRs, ofc...
20/ I posit the vast majority of this phenotype, #LMHRs (LDL ≥ 200, HDL ≥ 80, TG ≤ 70 -- see our papers, CholesterolCode.com/papers) are likely to present functional lipid metabolism, but more study is needed.
Regardless, they provide a truly unique opportunity to examine risk.
Regardless, they provide a truly unique opportunity to examine risk.
21/ If LDL (and ApoB) are independently atherogenic, then they are in very serious danger given their levels are in the very top 99% of the general population (>200 mg/dL) with some even in the top 99.9%.
Hence our longitudinal CCTA study w/ Lundquist (CitizenScienceFoundation.org/study)
Hence our longitudinal CCTA study w/ Lundquist (CitizenScienceFoundation.org/study)
22/ To reiterate what I said earlier, I know this conversation is a limited one because I've been having it for over 7 years.
Some folks see my experiments and/or my model and just "get" it -- or at least start asking the metabolic questions. (btw, @khurramn1 was most recent)
Some folks see my experiments and/or my model and just "get" it -- or at least start asking the metabolic questions. (btw, @khurramn1 was most recent)
23/ But for most, the causal chain model is attractive because it's easy to understand. One Lipoprotein To Rule Them All (is it ApoB? LDL? oxLDL? Glycated LDL? Small dense LDL? etc)
Discussing how all these can also be downstream of a broken lipid metabolism is complicated...
Discussing how all these can also be downstream of a broken lipid metabolism is complicated...
24/ ..& If there's any one thing it's taken me too long to learn, it's that there's a powerful gravitational pull toward models that simplify both the problems and their solutions.
Thank you to everyone who's made it this far. Hopefully I kept it lay-friendly enough this time 😃
Thank you to everyone who's made it this far. Hopefully I kept it lay-friendly enough this time 😃
• • •
Missing some Tweet in this thread? You can try to
force a refresh





