Interesting case of complicated acute bacterial rhinosinusitis in this child with no PMH presenting w/ HA, fever & L sided weakness
#NeuroTwitter #ent #radres #neurosurgery @TheASNR @ASHNRSociety @PhilipRChapman1 #radres #futureradres
#NeuroTwitter #ent #radres #neurosurgery @TheASNR @ASHNRSociety @PhilipRChapman1 #radres #futureradres




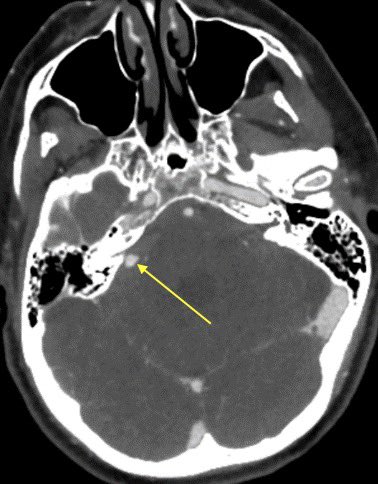
CT shows opacification of the frontal and anterior ethmoid sinuses without evidence of cortical dehiscence
💡 In peds, infection can spread through vascular channels w/o destroying the bone
💡 In peds, infection can spread through vascular channels w/o destroying the bone


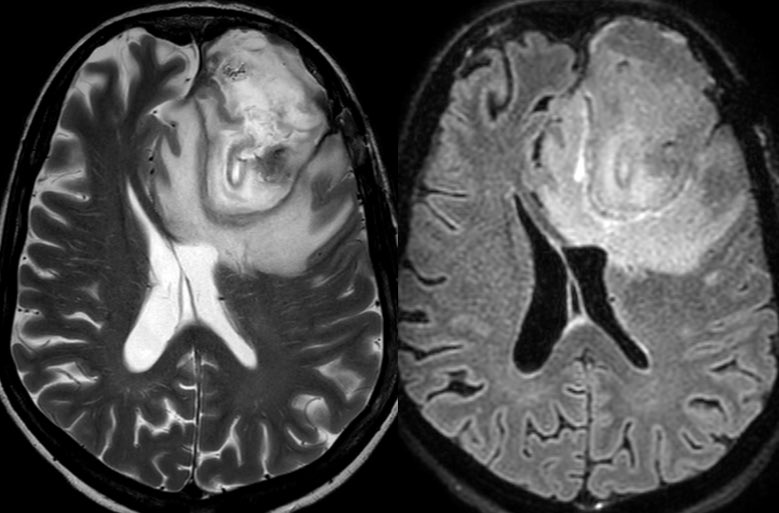
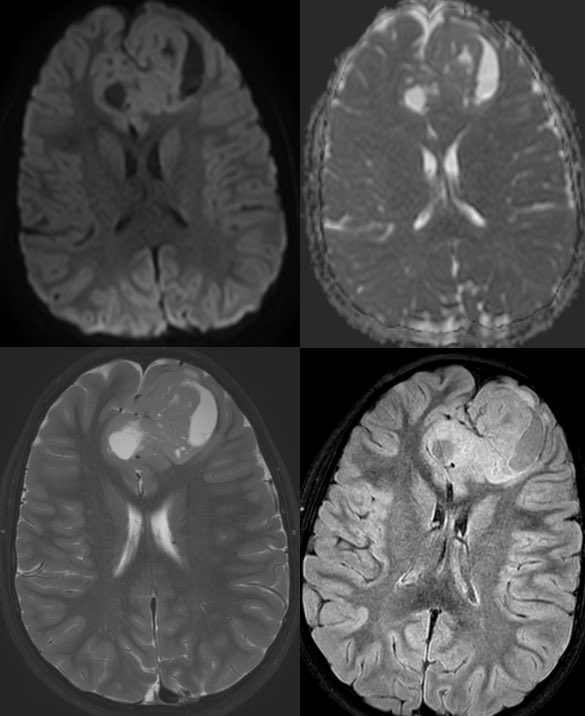
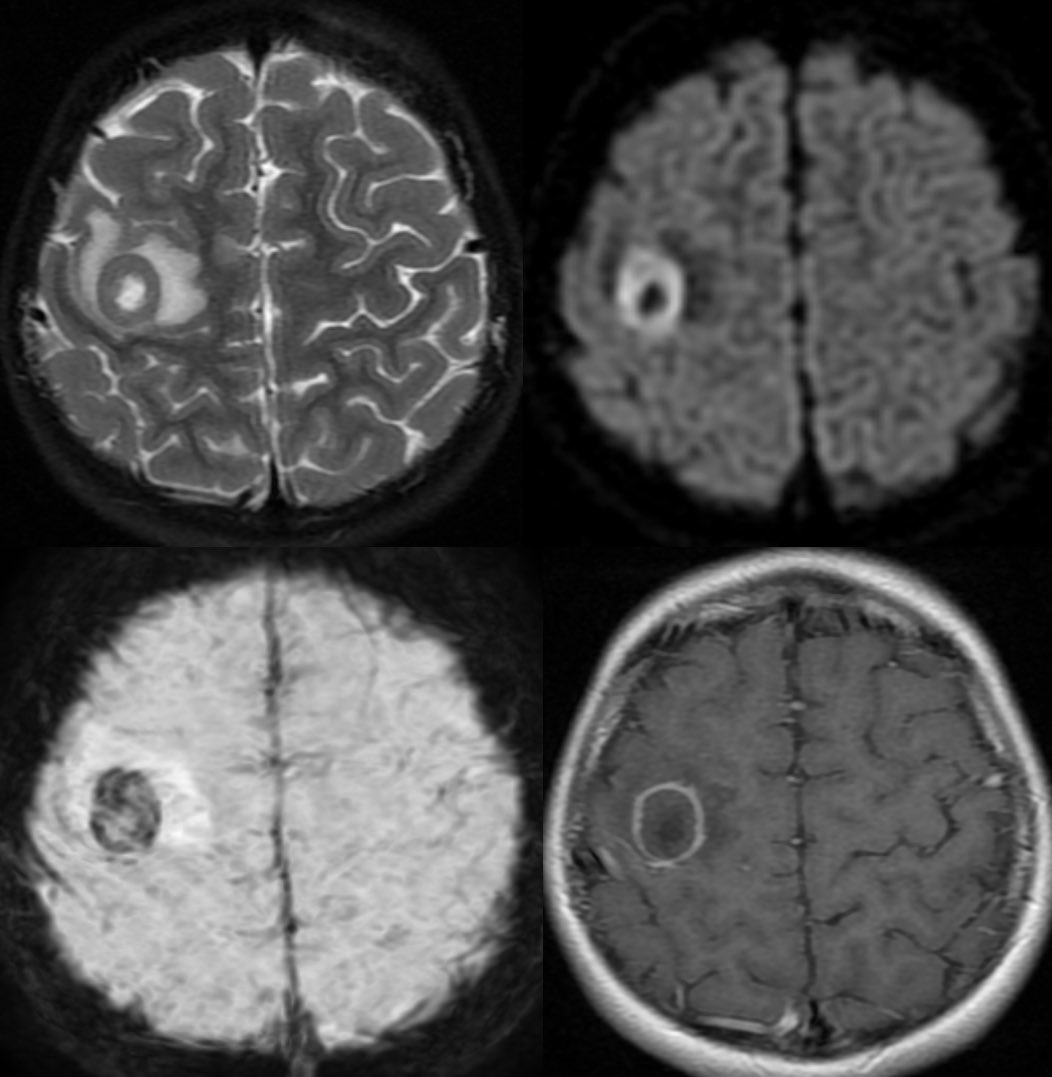
MR shows abnormal signal filling the sinuses with associated restricted diffusion 2/2 purulent material
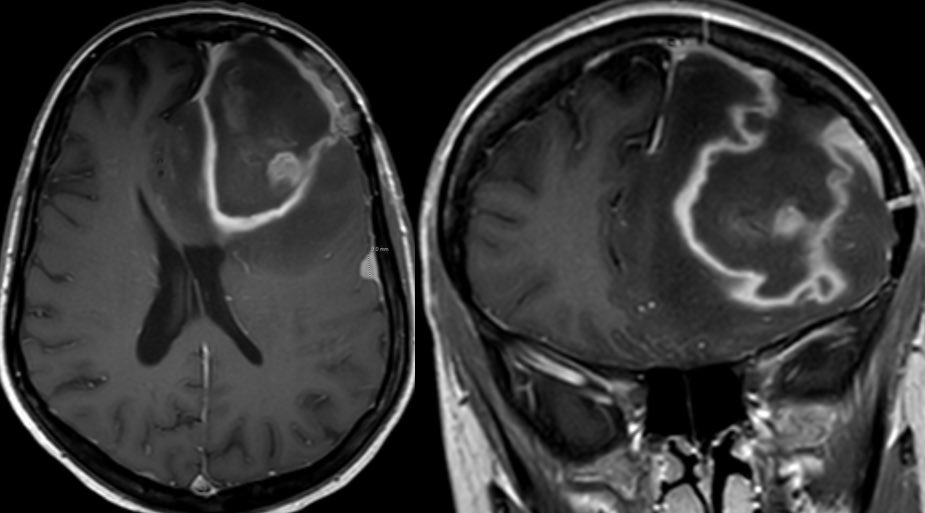
Post contrast we see areas of relative hypoenhancement in comparison to the normal mucosa on the contralateral side
Post contrast we see areas of relative hypoenhancement in comparison to the normal mucosa on the contralateral side



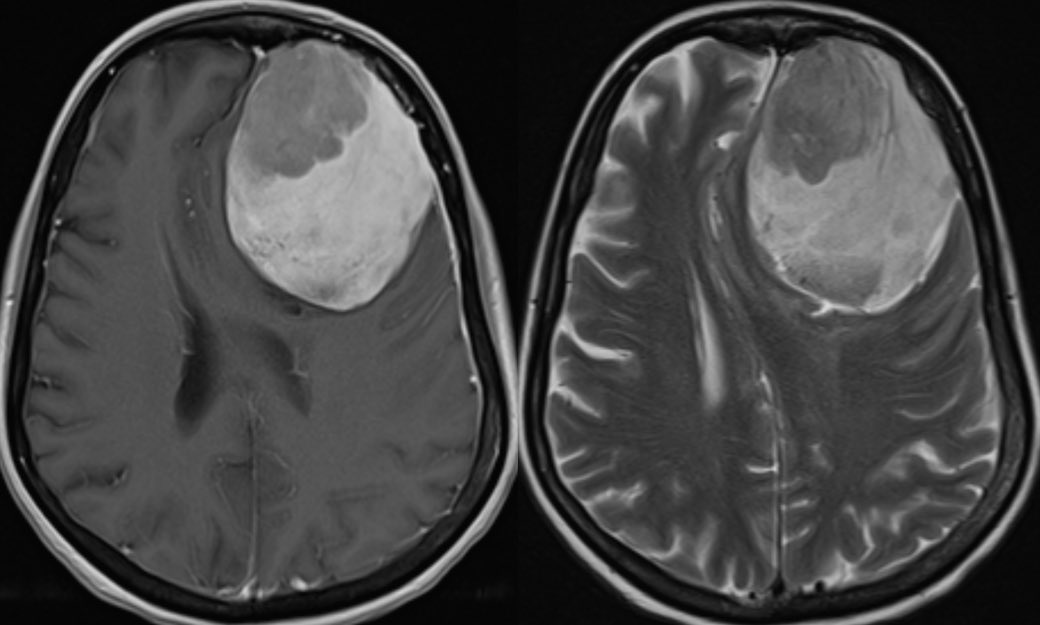
There is smooth pachymeningeal enhancement, suggestive of intracranial extension as well as an abscess in the right frontal lobe

Learning points:
💡 Acute sinusitis is a clinical diagnosis (imaging has poor correlation w/ symptoms as there is a high incidence of mucosal abnormalities in asymptomatic patients)
💡 Even normal sinus CT can have endoscopic evidence of sinusitis
💡 Acute sinusitis is a clinical diagnosis (imaging has poor correlation w/ symptoms as there is a high incidence of mucosal abnormalities in asymptomatic patients)
💡 Even normal sinus CT can have endoscopic evidence of sinusitis
💡 imaging can be used when complications are suspected
💡 CT sinuses can also be used in the outpatient setting in patients with chronic or recurrent sinusitis as a preoperative evaluation in those who may benefit from FESS
💡 CT sinuses can also be used in the outpatient setting in patients with chronic or recurrent sinusitis as a preoperative evaluation in those who may benefit from FESS
💡 Reduced or absent mucosal enhancement is NOT pathognomonic for invasive fungal sinusitis as it can be seen in mucoceles (possibly with superimposed infection) and patchy asymmetric diminished enhancement in bacterial sinusitis
Possible mechanism is increased sinus pressure leading to reduced perfusion or possible mucosal necrosis (if it can invade bone why not cause mucosal necrosis)? This is just speculation, I do not know what actually occurs 🤷🏻♂️
💡 Invasive fungal is usually thickened absent mucosal enhancement, no restricted diffusion, bone erosions and immunocompromised host
• • •
Missing some Tweet in this thread? You can try to
force a refresh