🔥 A deep dive into how Pfizer and their original mRNA manufacturer BioNTech prepared early for the pandemic that appeared to unfold into 2020...
#COVID19 #Covid #mrna @RobertKennedyJr @Johnincarlisle @delbigtree @AlexBerenson @benshapiro @elonmusk @KimIversenShow
1/n 🧵
#COVID19 #Covid #mrna @RobertKennedyJr @Johnincarlisle @delbigtree @AlexBerenson @benshapiro @elonmusk @KimIversenShow
1/n 🧵

9/4/2019
Bill #Gates invests 50 million euros in Biontech, a manufacturer of genetically engineered therapies for cancer patients.
investors.biontech.de/news-releases/…
Bill #Gates invests 50 million euros in Biontech, a manufacturer of genetically engineered therapies for cancer patients.
investors.biontech.de/news-releases/…

10/18/2019
The #Gates Foundation's Event 201 pandemic simulation game simulates a coronavirus outbreak in Brazil and recommends, among other things, consistent media control, algorithm manipulation and fact checking.
youtube.com/playlist?list=…
The #Gates Foundation's Event 201 pandemic simulation game simulates a coronavirus outbreak in Brazil and recommends, among other things, consistent media control, algorithm manipulation and fact checking.
youtube.com/playlist?list=…
11/2019 (undated)
The National Center for Medical Intelligence (NCMI) reports exceptional cases of illness in #Wuhan. The Pentagon denies it.
abcnews.go.com/Politics/intel…
The National Center for Medical Intelligence (NCMI) reports exceptional cases of illness in #Wuhan. The Pentagon denies it.
abcnews.go.com/Politics/intel…
11/14/2019
#Biontech would like to work on mRNA vaccines. #Sahin hopes for the first approval in 5-6 years.
#Biontech would like to work on mRNA vaccines. #Sahin hopes for the first approval in 5-6 years.
12/19 (undated)
The first clips - later to be found to be staged - from #Wuhan are appearing on social media.
The first clips - later to be found to be staged - from #Wuhan are appearing on social media.
12/31/2019
The first official reports on COVID. Peoples Daily China reports a novel lung disease in #Wuhan.
wap.peopleapp.com/article/498300…
The first official reports on COVID. Peoples Daily China reports a novel lung disease in #Wuhan.
wap.peopleapp.com/article/498300…
1/10/2020
Professor Edward Holmes posts a message by Prof. Yong-Zhen Zhang about the alleged novel viral genome.
To this date, the exact 'genome contigs' remain unreproducible and no assembler has ever found the entire genome from start to end.
usmortality.substack.com/p/sars-cov-2-g…
Professor Edward Holmes posts a message by Prof. Yong-Zhen Zhang about the alleged novel viral genome.
To this date, the exact 'genome contigs' remain unreproducible and no assembler has ever found the entire genome from start to end.
usmortality.substack.com/p/sars-cov-2-g…


1/22/2020
President #Trump comments on the coronavirus for the first time in Davos.
cnbc.com/2020/01/22/tru…
President #Trump comments on the coronavirus for the first time in Davos.
cnbc.com/2020/01/22/tru…
1/22/2020
The Johns Hopkins University starts its Covid Dashboard, just as practiced in even 201.
The Johns Hopkins University starts its Covid Dashboard, just as practiced in even 201.

1/23/2020
Prof. Dr. Drosten publishes the first PCR test protocol for the 'novel coronavirus' without having access to a real virus sample.
The publication was peer-reviewed in less than 24h, which is unheard of.
eurosurveillance.org/content/10.280…
Prof. Dr. Drosten publishes the first PCR test protocol for the 'novel coronavirus' without having access to a real virus sample.
The publication was peer-reviewed in less than 24h, which is unheard of.
eurosurveillance.org/content/10.280…

1/21/2020
The first US case, a man who went to an urgent care clinic "after seeing reports about the outbreak."
history.com/this-day-in-hi…
The first US case, a man who went to an urgent care clinic "after seeing reports about the outbreak."
history.com/this-day-in-hi…

3/11/2020 WHO officially declares a pandemic.
who.int/director-gener…
who.int/director-gener…
Lockdowns begin.
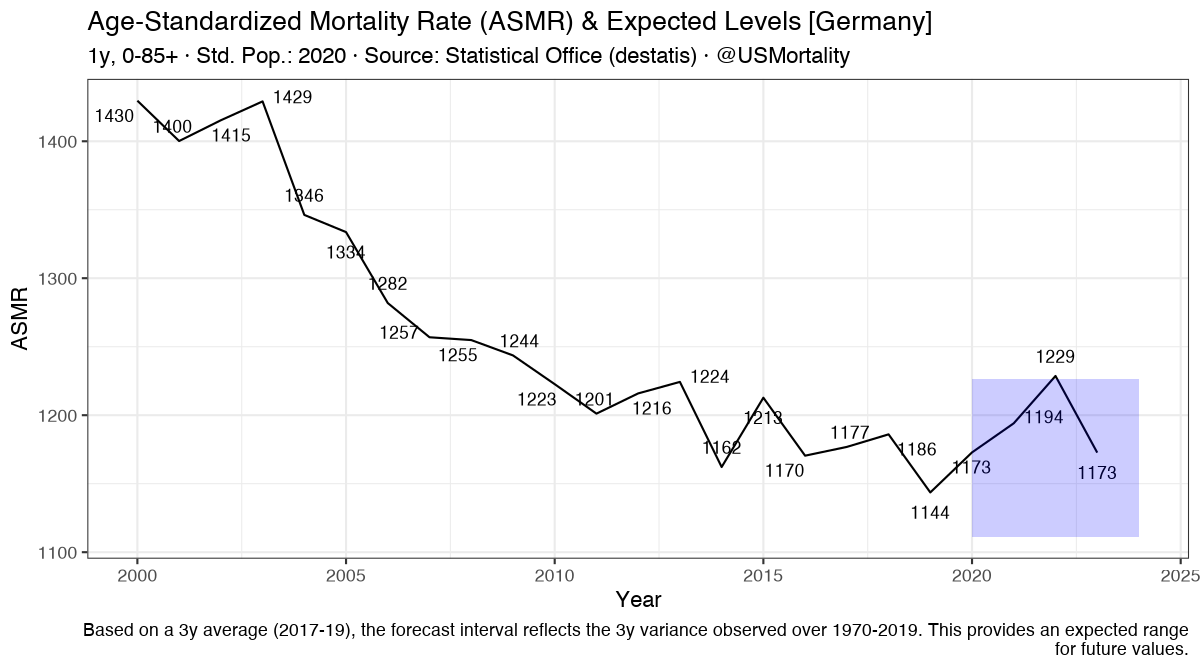
As economies come to a stop, and most people stay at home, mortality rises in certain places.
NYC experiences a rise of 5x normal mortality, while other cities see significantly less deaths.
As economies come to a stop, and most people stay at home, mortality rises in certain places.
NYC experiences a rise of 5x normal mortality, while other cities see significantly less deaths.

Dr. Rancourt concludes, that the initial peaks seen synchronously around the world are "from an epidemiological standpoint strictly impossible, because the time from seeding of the infection to the measurable rise in mortality is completely uncertain."
https://twitter.com/USMortality/status/1667410150364446722
3/25/2020
#Gates : "Ultimately, we need certificates."
#Gates : "Ultimately, we need certificates."
https://twitter.com/provoziert/status/1667215061058764812
During the covid pandemic, flu completely disappears.
To this date, the exact mechanism remains unclear.
To this date, the exact mechanism remains unclear.

7/30/2021
Dr. Fauci, stating on national TV, that vaccinated people are “capable of transmitting the infection” and stating that the level of virus are “essentially equivalent” between vaccinated and unvaccinated infected people.
Dr. Fauci, stating on national TV, that vaccinated people are “capable of transmitting the infection” and stating that the level of virus are “essentially equivalent” between vaccinated and unvaccinated infected people.
8/6/2021
In a COVID-19 "outbreak" in Barnstable County, MA - CDC confirms that "Cycle threshold values were similar among specimens from patients who were fully vaccinated and those who were not." therefore not offering any protection against spread.
cdc.gov/mmwr/volumes/7…
In a COVID-19 "outbreak" in Barnstable County, MA - CDC confirms that "Cycle threshold values were similar among specimens from patients who were fully vaccinated and those who were not." therefore not offering any protection against spread.
cdc.gov/mmwr/volumes/7…
6/2023
Yet, 3 year later:
"The WHO will take up the EU system of digital COVID-19 certification to establish a global system that will help protect citizens across the world from on-going and future health threats, including pandemics."
commission.europa.eu/strategy-and-p…
Yet, 3 year later:
"The WHO will take up the EU system of digital COVID-19 certification to establish a global system that will help protect citizens across the world from on-going and future health threats, including pandemics."
commission.europa.eu/strategy-and-p…
H/T, for many of the tweets in German: @provoziert
@EWoodhouse7
Find my latest work on all-cause mortality at: mortality.watch
@EWoodhouse7
Find my latest work on all-cause mortality at: mortality.watch
• • •
Missing some Tweet in this thread? You can try to
force a refresh