1/10 “To PCI, or Not to PCI, That is the Question” Will Shakespeare, MD
#FITSurvivalGuide
*Per many contentious #cardiotwitter discussions I realize this is loaded topic but I’m going to attempt an early stage #ACCFIT overview while recognizing there is a lot of nuance.
#FITSurvivalGuide
*Per many contentious #cardiotwitter discussions I realize this is loaded topic but I’m going to attempt an early stage #ACCFIT overview while recognizing there is a lot of nuance.

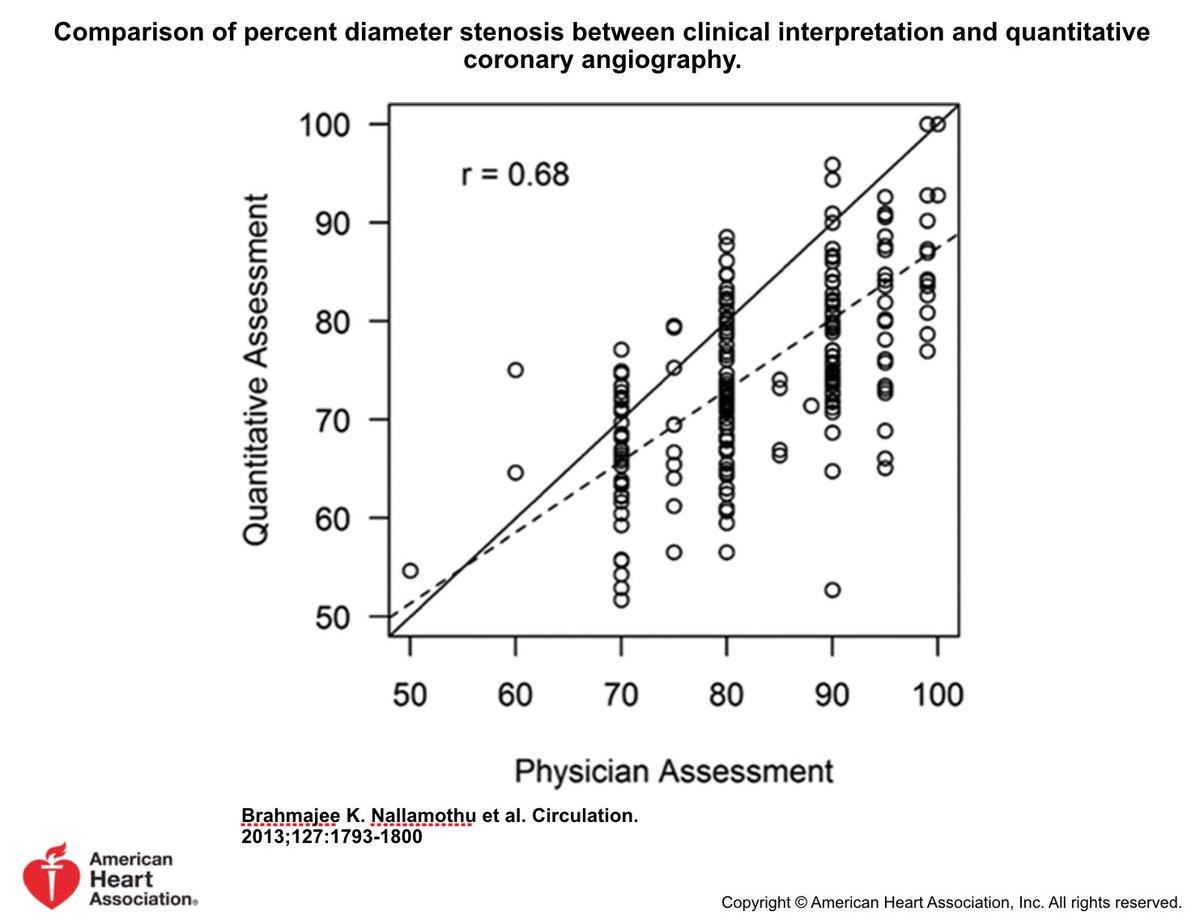
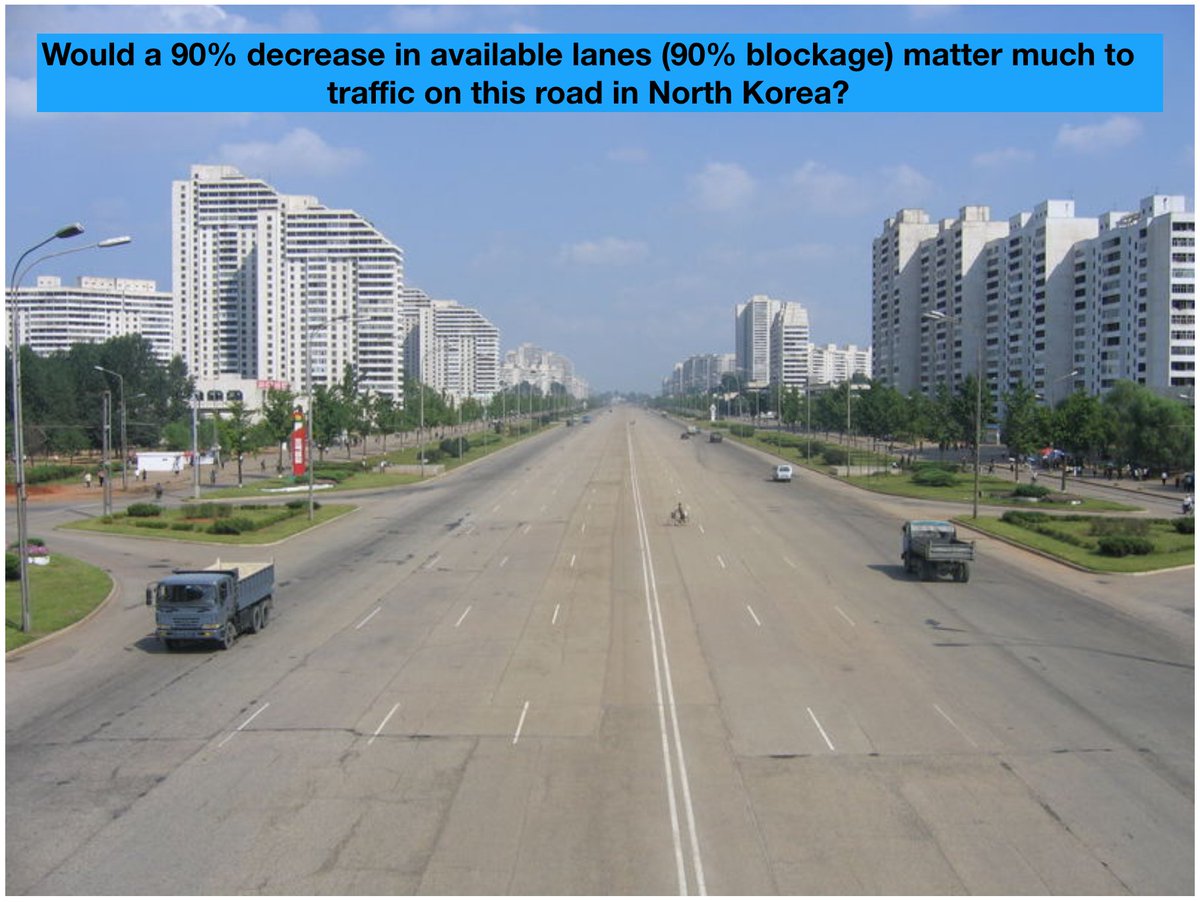
2/10 Why not “See lesion Fix lesion”?
Poor correlation between est'd visual stenosis & quantitative stenosis. And, without noninvasive ischemic data, coronary angio has limited accuracy w/ regard to identifying significance of many stenoses
*STEMI PCI already done @KhandelwalMD
Poor correlation between est'd visual stenosis & quantitative stenosis. And, without noninvasive ischemic data, coronary angio has limited accuracy w/ regard to identifying significance of many stenoses
*STEMI PCI already done @KhandelwalMD
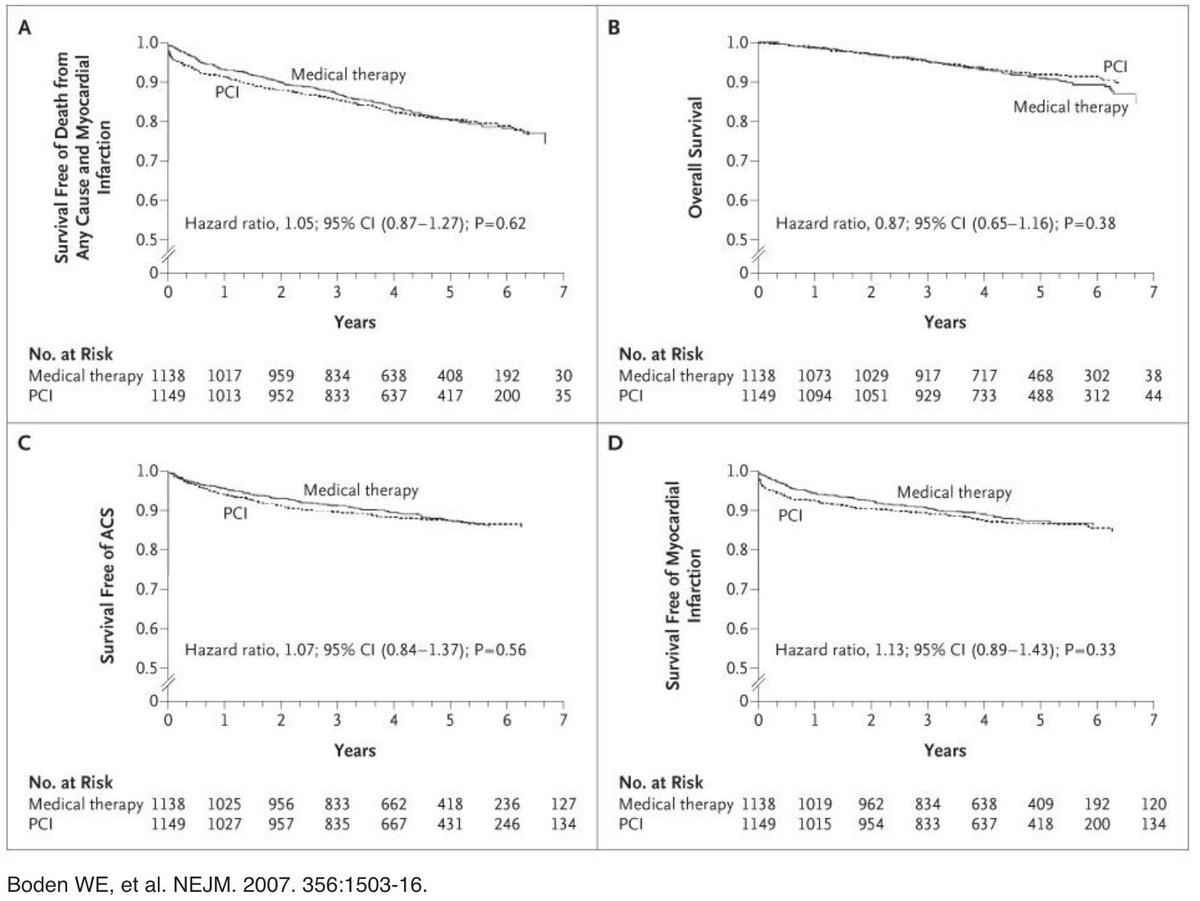
3/10 COURAGE trial (OMT vs OMT and PCI of visually-estimated significant stenoses): No difference death/MI between OMT & OMT/PCI. PCI demonstrated clinical benefit only when treating relevant myocardial ischemia determined by noninvasive testing.

4/10 If no non-invasive testing available prior to LHC?
FFR: Ratio of max blood flow in stenotic artery to normal max blood flow (calculate simultaneous ratio distal coronary pressure to aortic pressure: Pd/Pa).
Normal FFR: 1.0 & FFR <0.80 is significant for ischemia.
FFR: Ratio of max blood flow in stenotic artery to normal max blood flow (calculate simultaneous ratio distal coronary pressure to aortic pressure: Pd/Pa).
Normal FFR: 1.0 & FFR <0.80 is significant for ischemia.


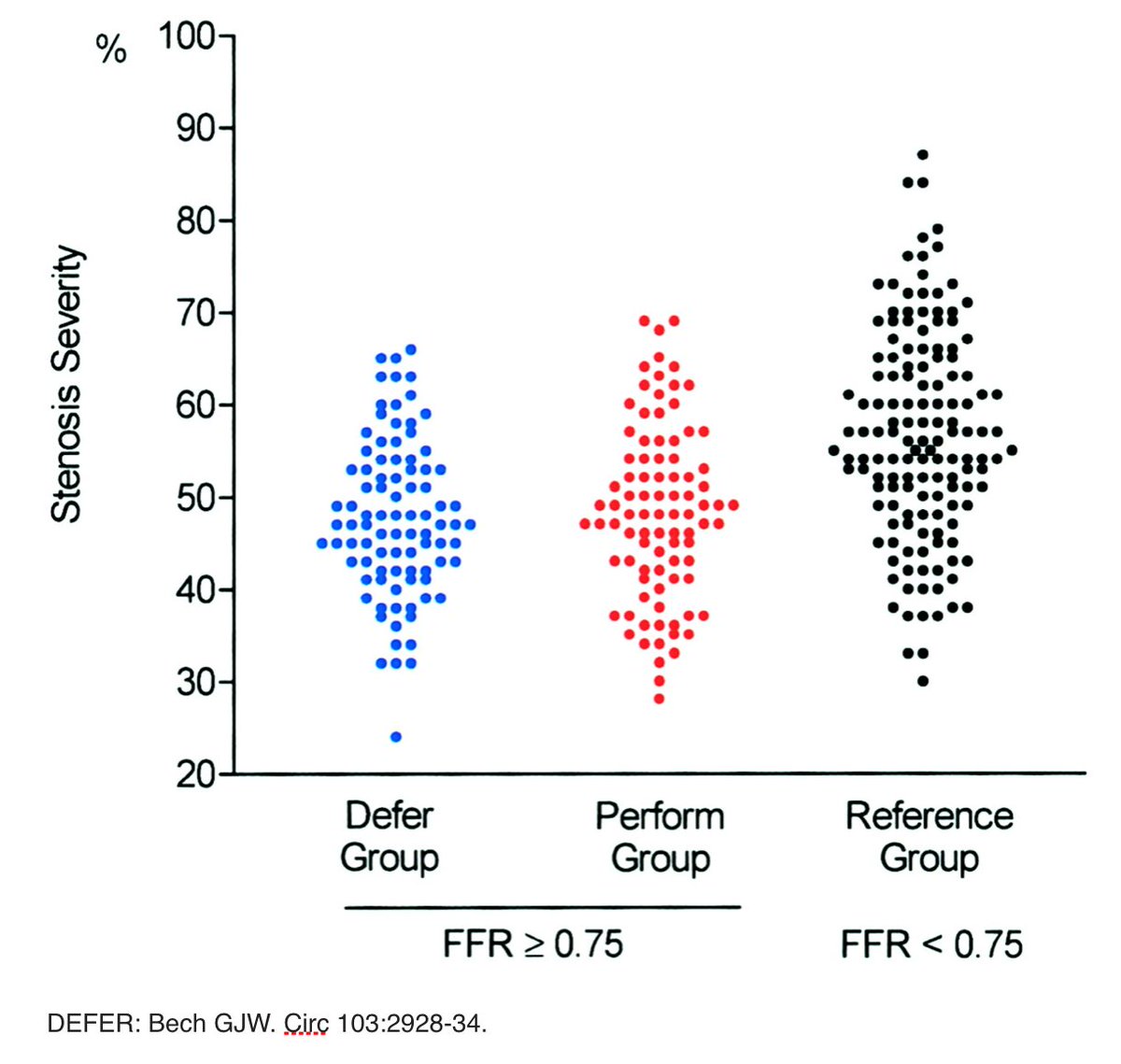
5/10 DEFER: Prognosis of non-FFR sig vessels is excellent & PCI of non-FFR sig vessels does no benefit
FAME: FFR-guided PCI reduces death, nonfatal MI, repeat revasc compared to angio-guided PCI
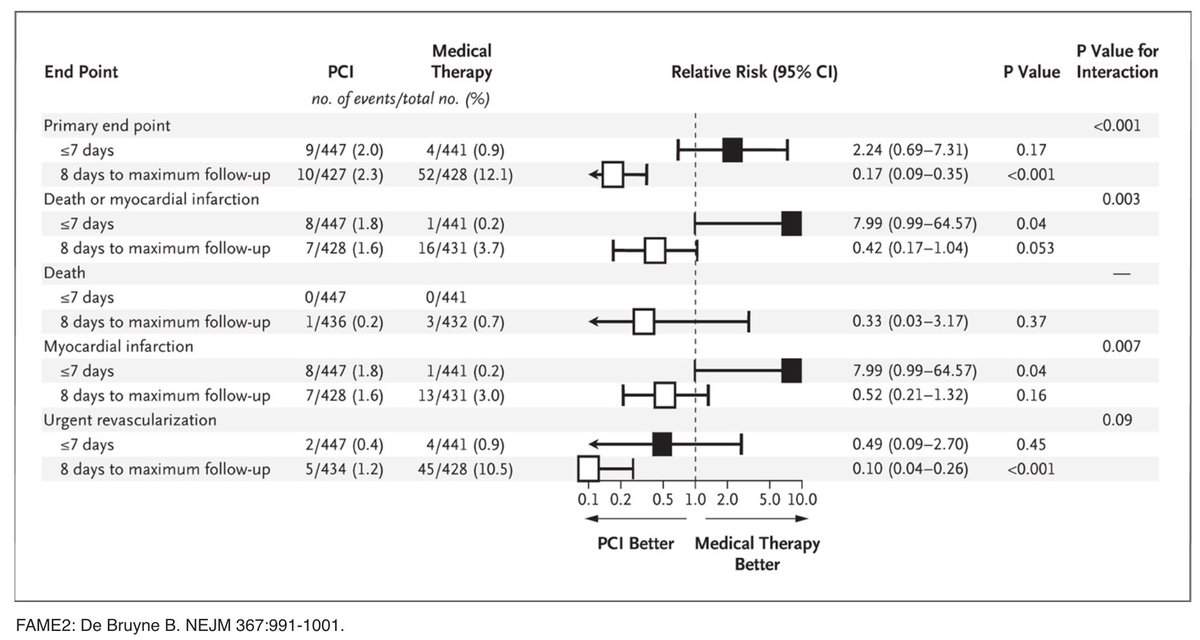
FAME 2: PCI for sig FFR reduces death, nonfatal MI, urgent revise compared to OMT
FAME: FFR-guided PCI reduces death, nonfatal MI, repeat revasc compared to angio-guided PCI
FAME 2: PCI for sig FFR reduces death, nonfatal MI, urgent revise compared to OMT


6/10 Instantaneous free-Wave Ratio (iFR) - non inferior to FFR in 2 large randomized trials: DEFINE FLAIR and iFR-Swedeheart



7/10 Real-world case study to try to tie this all together
70yo f smoker w/ htn, HL referred for LHC to eval DOE. ECG/echo nl. ETT stopped 4 min s/t DOE. Lexi SPECT: multi small mild/mod reversible abnormalities: apical anterior, mid inferior, mid anterolateral, inferolateral.
70yo f smoker w/ htn, HL referred for LHC to eval DOE. ECG/echo nl. ETT stopped 4 min s/t DOE. Lexi SPECT: multi small mild/mod reversible abnormalities: apical anterior, mid inferior, mid anterolateral, inferolateral.

8a/10 how would you treat? (Poll follows angiograms) #RadialFirst @mikevalentineMD @DickKovacs @AAllenSeals @RickChazal @cardio10s @ditchhaporia @bowalpole @HadleyWilsonMD
What would you do next?
9/10 Given multiple small/mod areas of ischemia in multiple territories on SPECT, I opted for choice D. iFR demonstrated no indication for PCI.
dLAD 0.95
dLCx 0.98
dRCA 0.98
*if distal vessel iFR <0.90 I would have done serial lesion analysis to determine exactly where to tx
dLAD 0.95
dLCx 0.98
dRCA 0.98
*if distal vessel iFR <0.90 I would have done serial lesion analysis to determine exactly where to tx


10/10 Ultimately, you have to do what is best for each pt. Judicious PCI is a must. Fellowship is about honing the decision-making skills to decide when to intervene.
I’m humbled to have been asked to participate w/ #FITSurvivalGuide. Good luck #ACCFIT!
I’m humbled to have been asked to participate w/ #FITSurvivalGuide. Good luck #ACCFIT!