#FITSurvivalGuide Aortic Emergency style!
Will discuss presentation/dx/complications/tx for:
1. Aortic dissection💉
2. IMH❣️
3. PAU
4. Traumatic transection
5. Non-emergent aneurysm surgical cutoffs (because boards loves them!)
Hoping @keaglemd can share his expertise as well!
Will discuss presentation/dx/complications/tx for:
1. Aortic dissection💉
2. IMH❣️
3. PAU
4. Traumatic transection
5. Non-emergent aneurysm surgical cutoffs (because boards loves them!)
Hoping @keaglemd can share his expertise as well!
Everyone please feel free to add to this thread for more learning #FIT #CardioEd
@dr_chirumamilla @APostalian @heartdoc45 @Babar_Basir @DrJayMohan @SamRRazaMD @DocStrom @DocSavageTJU @SamRRazaMD @DrQuinnCapers4 @cardiojaydoc02 @DrSheilaSahni @saraceciliamtz @onco_cardiology
@dr_chirumamilla @APostalian @heartdoc45 @Babar_Basir @DrJayMohan @SamRRazaMD @DocStrom @DocSavageTJU @SamRRazaMD @DrQuinnCapers4 @cardiojaydoc02 @DrSheilaSahni @saraceciliamtz @onco_cardiology
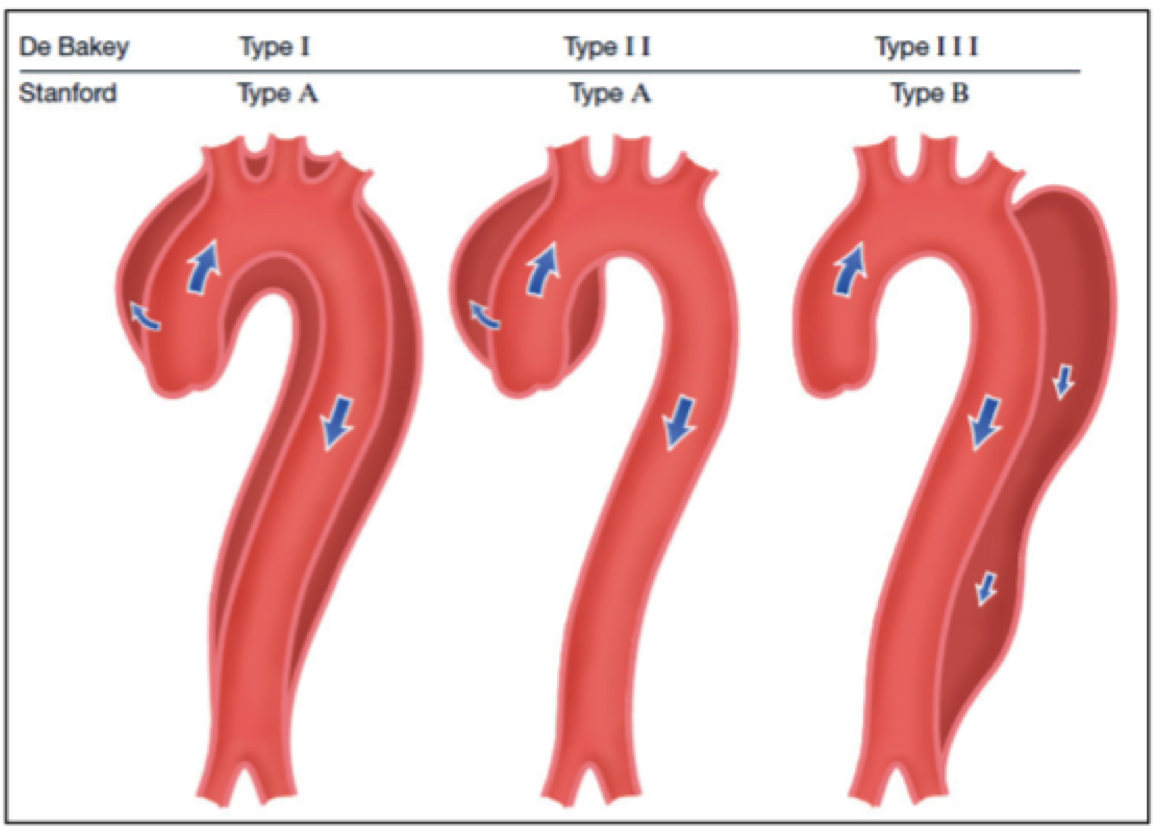
1/ Dreaded DISSECTION!
DeBakey and Stanford class⬇️
RFs: HTN, Male, age
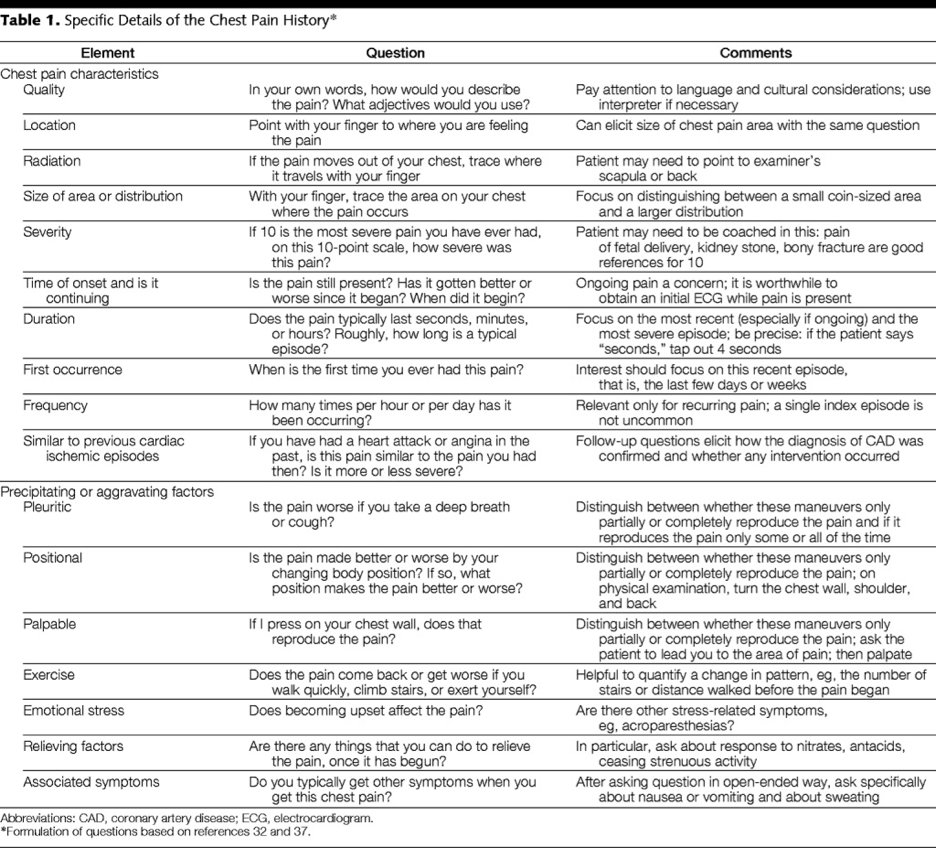
Presents: Abrupt severe pain (chest or back)! Check both💪 BP
Dx: CTA>TEE>TTE
Complications: Propagation 2 RCC/RCA MI (think b4 going to cath lab!) pericardial eff (but try to avoid pericardiocentesis!)
DeBakey and Stanford class⬇️
RFs: HTN, Male, age
Presents: Abrupt severe pain (chest or back)! Check both💪 BP
Dx: CTA>TEE>TTE
Complications: Propagation 2 RCC/RCA MI (think b4 going to cath lab!) pericardial eff (but try to avoid pericardiocentesis!)
2/ Dissection Treatment: varies with type! In general IV BB⬇️ shear wall stress &⬇️propagation.
Type A: ✂️ASAP! Mortality increases with⌚️
Type B, complicated (continued pain/rupture/rapid expansion): TEVAR>✂️
Type B, uncomplicated: Lifelong💊, surveillance
Dont do ⬇️
Type A: ✂️ASAP! Mortality increases with⌚️
Type B, complicated (continued pain/rupture/rapid expansion): TEVAR>✂️
Type B, uncomplicated: Lifelong💊, surveillance
Dont do ⬇️

3/Intramural hematoma❣️
Rupture of vasa vasorum (no flap!)
RFs/Presentation: similar to dissection!
~20% progress to dissection (ascending>descending)
Dx: CTA/TEE
Tx: typically ✂️for ascending
Complications: periaortic hematoma/effusion/AI
Rupture of vasa vasorum (no flap!)
RFs/Presentation: similar to dissection!
~20% progress to dissection (ascending>descending)
Dx: CTA/TEE
Tx: typically ✂️for ascending
Complications: periaortic hematoma/effusion/AI

4/ Penetrating aortic ulcer (PAU💥)
Ulcerated plaque penetrates aortic wall
RFs: CAD/PAD,🚬
Presenation: Usually nagging pain (like aneurysm)
Dx: CTA (also MRI/TEE). Most commonly DESCENDING aorta
Ulcerated plaque penetrates aortic wall
RFs: CAD/PAD,🚬
Presenation: Usually nagging pain (like aneurysm)
Dx: CTA (also MRI/TEE). Most commonly DESCENDING aorta

5/ Tx: Depends on extent of lesion. Treat underlying atherosclerosis if localized & consider EVAR
Complications: Can lead 2 rupture!
Complications: Can lead 2 rupture!

6/ Traumatic aortic transection
RF: Bad luck😞
Tear typically at prox desc aorta, near L subclavian a due to tethering of the aorta by the ligamentum arteriosum
Presentation: 🚗accident/decel injury, severe pain &/or shock from bleeding. most☠️if fully transected
Dx: Hx/CTA/TEE
RF: Bad luck😞
Tear typically at prox desc aorta, near L subclavian a due to tethering of the aorta by the ligamentum arteriosum
Presentation: 🚗accident/decel injury, severe pain &/or shock from bleeding. most☠️if fully transected
Dx: Hx/CTA/TEE

7/ Traumatic Transection Tx: ✂️ASAP & supportive measures until surgery! Unclear role for endovascular intervention.
PSA: Don't drive fast and wear your seatbelt!🧐
PSA: Don't drive fast and wear your seatbelt!🧐
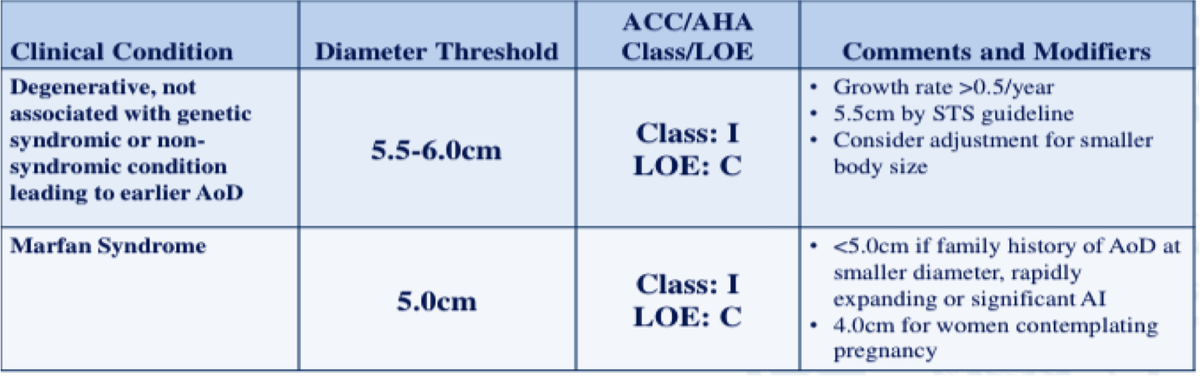
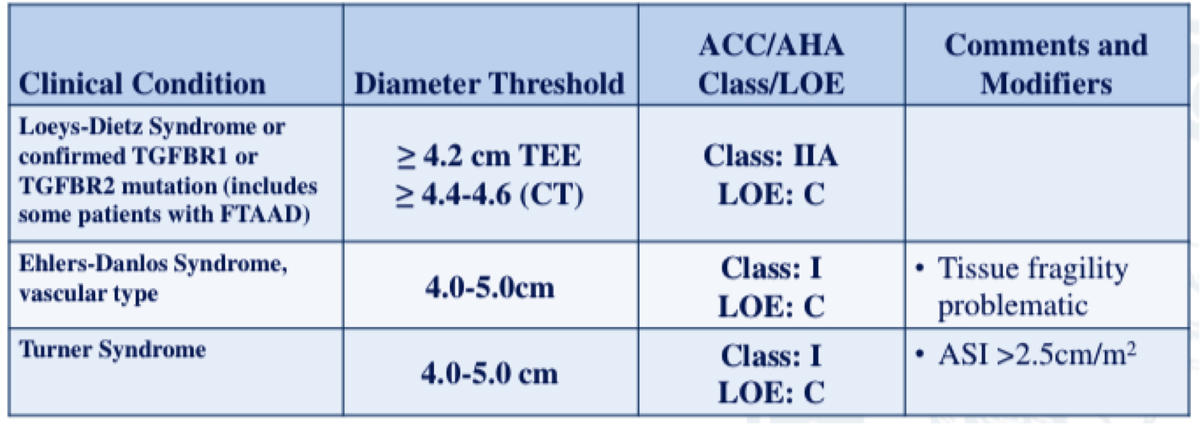
8/ Last but not least, briefly thoracic & abd aortic aneurysms-- bc @ACCCardioEd boards❣️them & we need to know for our patients!
Thoracic: Always 🤨 underlying conn tissue d/o or bicuspid valve!
Presents: usually asymptomatic until rupture!
Dx: CTA/TTE/TEE
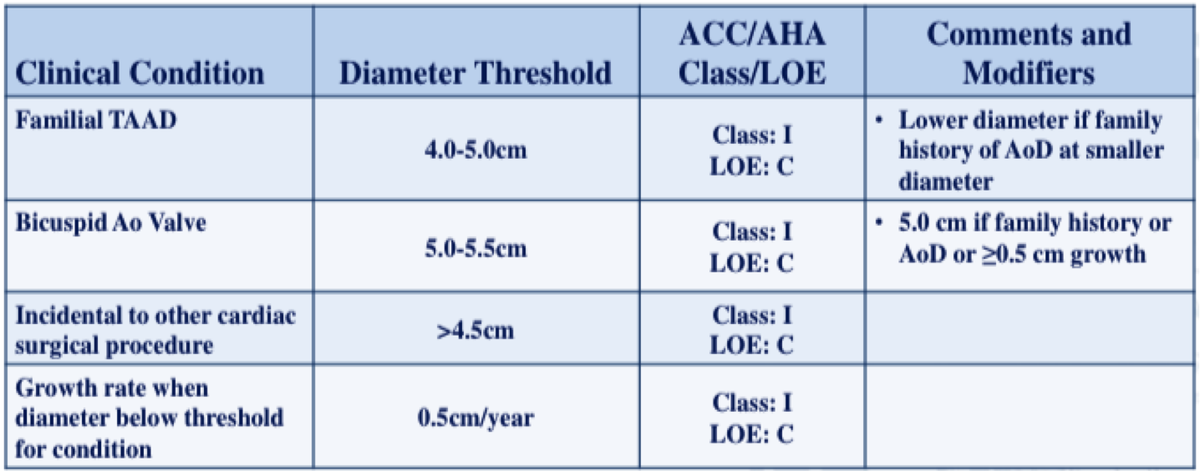
✂️cutoffs⬇️
Thoracic: Always 🤨 underlying conn tissue d/o or bicuspid valve!
Presents: usually asymptomatic until rupture!
Dx: CTA/TTE/TEE
✂️cutoffs⬇️
9/ Abdominal aneurysm
RF: 🚬, HTN, male
Presents: again, asymptomatic until rupture!
Screen (males) who have ever smoked ~100 cigarettes!
Monitor: CT or US q6 mos if >4cm
Tx: Surgery/EVAR in general >5.4cm (consider 5.0cm for female) or if symptomatic!
RF: 🚬, HTN, male
Presents: again, asymptomatic until rupture!
Screen (males) who have ever smoked ~100 cigarettes!
Monitor: CT or US q6 mos if >4cm
Tx: Surgery/EVAR in general >5.4cm (consider 5.0cm for female) or if symptomatic!

That's all folks! Please fill in any gaps or thoughts and I hope this is helpful! Special shoutout to @dr_chirumamilla for putting the #FITSurvivalGuide together! So glad to be a part of it!